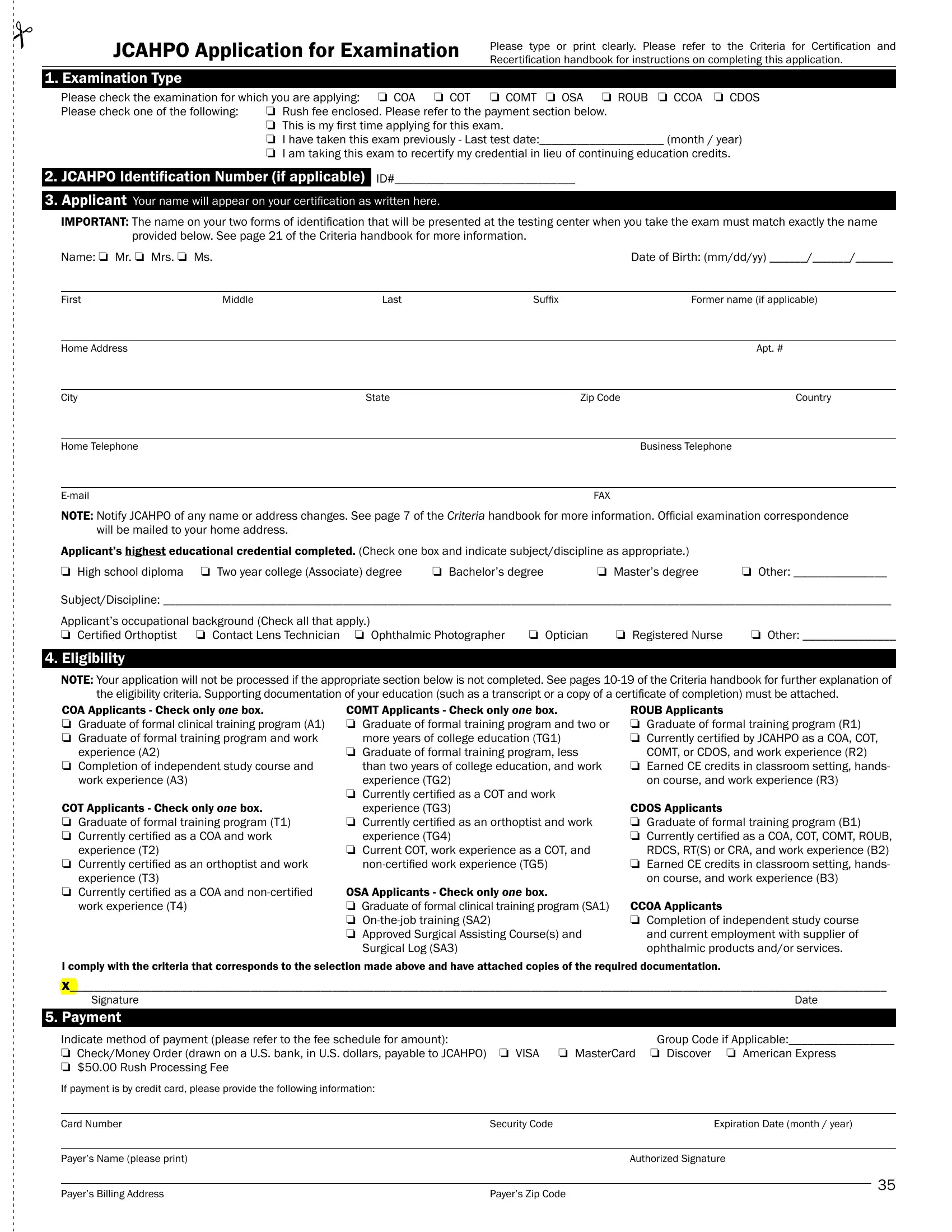
The journey toward certification in the ophthalmic medical field is marked by an essential step: filling out the JCAHPO Application for Examination form. This meticulously designed form serves as the gateway for professionals aiming to validate their expertise across various specialties, including Certified Ophthalmic Assistant (COA), Certified Ophthalmic Technician (COT), and several others, through the Joint Commission on Allied Health Personnel in Ophthalmology (JCAHPO). Applicants are instructed to fill out the form with precise details such as examination type, personal identification, educational background, and employment information, ensuring the accuracy to match the identification presented at testing centers. The application delves into eligibility criteria linked to educational and occupational background, requiring supporting documentation for verification. Furthermore, it outlines payment methods, underscoring the option for expedited processing and highlights the responsibility agreement that underscores ethical conduct and respect for confidential examination content. With a focus on compliance with the Americans with Disabilities Act (ADA), the form also accommodates candidates requiring special examination conditions, ensuring inclusivity. Prospective candidates are guided to complete the application with attention to verifying their eligibility, securing a sponsor or employer endorsement, and fulfilling specific prerequisites for their targeted certification. The process concludes with an agreement towards maintaining the integrity of the certification pursuit, emphasizing the form’s pivotal role in the journey toward achieving and maintaining professional certification in the ophthalmic field.
| Question | Answer |
|---|---|
| Form Name | Jcahpo Application For Examination Form |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | Ophthalmic, ADA, Orthoptist, OSA |
JCAHPO Application for Examination |
Please type or print clearly. Please refer to the Criteria for Certiication and |
|
Recertiication handbook for instructions on completing this application. |
1. Examination Type
Please check the examination for which you are applying: o COA o COT o COMT o OSA o ROUB o CCOA o CDOS
Please check one of the following: o Rush fee enclosed. Please refer to the payment section below.
oThis is my irst time applying for this exam.
oI have taken this exam previously - Last test date:____________________ (month / year)
oI am taking this exam to recertify my credential in lieu of continuing education credits.
2.JCAHPO Identiication Number (if applicable)_ ID#_____________________________
3.Applicant Your name will appear on your certiication as written here.
IMPORTANT: The name on your two forms of identiication that will be presented at the testing center when you take the exam must match exactly the name provided below. See page 21 of the Criteria handbook for more information.
Name: o Mr. o Mrs. o Ms. |
|
|
|
Date of Birth: (mm/dd/yy) ______/______/______ |
|
|
|
|
|
First |
Middle |
Last |
Sufix |
Former name (if applicable) |
|
|
|
|
|
Home Address |
|
|
|
Apt. # |
|
|
|
|
|
City |
|
State |
Zip Code |
Country |
|
|
|
|
|
Home Telephone |
|
|
|
Business Telephone |
|
|
|
|
|
|
|
FAX |
|
NOTe: Notify JCAHPO of any name or address changes. See page 7 of the Criteria handbook for more information. Oficial examination correspondence will be mailed to your home address.
Applicant’s highest educational credential completed. (Check one box and indicate subject/discipline as appropriate.)
o High school diploma o Two year college (Associate) degree o Bachelor’s degree o Master’s degree o Other: _______________
Subject/Discipline: _____________________________________________________________________________________________________________________
Applicant’s occupational background (Check all that apply.) |
|
|
|
|
o Certiied Orthoptist |
o Contact Lens Technician o Ophthalmic Photographer |
o Optician |
o Registered Nurse |
o Other: _______________ |
4. eligibility
NOTe: Your application will not be processed if the appropriate section below is not completed. See pages
COA Applicants - Check only ONE box. |
COMT Applicants - Check only ONE box. |
ROUB Applicants |
o Graduate of formal clinical training program (A1) |
o Graduate of formal training program and two or |
o Graduate of formal training program (R1) |
o Graduate of formal training program and work |
more years of college education (TG1) |
o Currently certiied by JCAHPO as a COA, COT, |
experience (A2) |
o Graduate of formal training program, less |
COMT, or CDOS, and work experience (R2) |
o Completion of independent study course and |
than two years of college education, and work |
o Earned CE credits in classroom setting, hands- |
work experience (A3) |
experience (TG2) |
on course, and work experience (R3) |
COT Applicants - Check only ONE box. |
o Currently certiied as a COT and work |
|
experience (TG3) |
CDOS Applicants |
|
o Graduate of formal training program (T1) |
o Currently certiied as an orthoptist and work |
o Graduate of formal training program (B1) |
o Currently certiied as a COA and work |
experience (TG4) |
o Currently certiied as a COA, COT, COMT, ROUB, |
experience (T2) |
o Current COT, work experience as a COT, and |
RDCS, RT(S) or CRA, and work experience (B2) |
o Currently certiied as an orthoptist and work |
o Earned CE credits in classroom setting, hands- |
|
experience (T3) |
|
on course, and work experience (B3) |
o Currently certiied as a COA and |
OSA Applicants - Check only ONE box. |
|
work experience (T4) |
o Graduate of formal clinical training program (SA1) |
CCOA Applicants |
|
o |
o Completion of independent study course |
|
o Approved Surgical Assisting Course(s) and |
and current employment with supplier of |
|
Surgical Log (SA3) |
ophthalmic products and/or services. |
I comply with the criteria that corresponds to the selection made above and have attached copies of the required documentation.
X____________________________________________________________________________________________________________________________________________
Signature |
Date |
5. Payment
Indicate method of payment (please refer to the fee schedule for amount): |
Group Code if Applicable:_________________ |
o Check/Money Order (drawn on a U.S. bank, in U.S. dollars, payable to JCAHPO) o VISA |
o MasterCard o Discover o American Express |
o $50.00 Rush Processing Fee |
|
If payment is by credit card, please provide the following information:
Card Number |
Security Code |
Expiration Date (month / year) |
|
|
|
|
|
Payer’s Name (please print) |
|
Authorized Signature |
|
|
|
|
|
|
|
|
35 |
Payer’s Billing Address |
Payer’s Zip Code |
|
|
|
|
||
|
|
|
|
JCAHPO Application for Examination
6. Responsibility Statement
JCAHPO's Responsibility for Certiication and Recertiication of Medical Personnel Performing Technical Ophthalmic Services for Ophthalmologists
JCAHPO is the federated organization of ophthalmological societies and associations which has been charged with certain responsibilities related to the education and utilization of allied health personnel in ophthalmology. To implement these goals, JCAHPO has established criteria for training, examination, certiication, and
utilization at various levels of expertise for ophthalmic medical personnel.
Certiication by JCAHPO indicates ONLY that the individual has fulilled the eligibility requirements and successfully completed an examination for which the individual qualiies. Certiication by JCAHPO does NOT imply, by any criteria, that the individual is qualiied as an independent practitioner.
AGReeMeNT OF CeRTIFICATION AND ReCeRTIFICATION
As an applicant for certiication or recertiication from JCAHPO, I agree to the following:
Numbers 1 and 2 applicable to COA, COT, COMT, OSA, CDOS, and ROUB applicants only.
1.I shall perform, to the best of my ability, those technical ophthalmic services speciically delegated to me by a sponsoring ophthalmologist/physician according to his or her directions, instructions, and prescriptions.
2.I shall provide technical ophthalmic services only in the ofice of my sponsoring ophthalmologist/physician, a medical clinic, or other medical facility.
Number 3 applicable to CCOA applicants only
3.I am currently employed by a corporation that does business within the ophthalmic community and, in my position, I will be interacting with ophthalmic professionals on a continuing basis.
Numbers
4.I authorize JCAHPO to communicate any violation of its rules or standards by me, my status of application or certiication, and any matter involving me to state and federal authorities, employers, training programs, and others.
5.I agree not to make and to correct immediately any statements concerning my certiication status which are or which become untrue or misleading. I agree to provide JCAHPO conirmation as requested by JCAHPO.
6.I release JCAHPO, its oficers, directors, agents, employers, committee members, and others for disciplinary action taken in good faith pursuant to the rules, standards, procedures, and sanctions of JCAHPO.
7.I authorize JCAHPO in its discretion to request information concerning matters relevant to this application and my certiication, recertiication, and review of certiication.
8.I have received and read the rules, standards, procedures and sanctions of JCAHPO. I comply with and agree to be bound by them.
9. Please respond to the following questions:
o Yes |
o No |
Have you ever had a certiication or license suspended or revoked? |
o Yes |
o No |
Have you ever been dismissed from a job because of alcohol or other drug dependency? |
o Yes |
o No |
Have you ever been convicted of a crime? |
If the answer to any question in Number 9 is "Yes,” include a statement of explanation with the application.
10.JCAHPO examinations are conidential and proprietary. The examination(s) are available to you, the examinee, soley for the purpose of assessing your proiciency level in the content areas referenced in the examination(s) for which you are eligible. You are expressly prohibited from disclosing, publishing, reproducing, or transmitting the examination(s) in any matter, in whole or in part, in any form or by any means, verbal or written, electronic or mechanical, for any purpose. By signing this application you agree to the above disclosure statement. If you do not agree to the disclosure statement and do not sign the application you will not be eligible to take any JCAHPO examinations.
I afirm that all statements made in the above application are true. (Sign and date below.)
X
Applicant’s Signature |
Date |
36
JCAHPO Application for Examination
7. Employer
All applicants, other than CCOA applicants, complete section A. CCOA applicants complete section B.
SeCTION A (for COA, COT, COMT, OSA, ROUB, and CDOS applicants)
Clinic Name
Clinic Address |
|
|
City |
|
State |
Zip |
|
|
|
|
|
|
|
Telephone |
|
|
|
FAX |
|
|
|
|
|
|
|
|
|
Clinic Manager |
First |
|
|
M.I. |
Last |
|
Employer’s Practice Setting (Check all that apply) |
|
|
|
|
|
|
o Private, Solo |
o Private, Group: Number of Physicians o |
o |
|
|
||
o Hospital Clinic or HMO |
o University Clinic |
o Other:______________________ |
|
|
||
employer’s Main Subspecialty (Check only one) |
|
|
|
|
|
|
o Cataract and IOL |
|
o Comprehensive Ophthalmology o Contact Lenses |
o Cornea and External Diseases |
|||
o Glaucoma |
|
o Low Vision |
o |
o Ophthalmic Pathology |
|
|
o Ophthalmic Plastic/Reconstructive Surgery |
o Optical Dispensing |
o Pediatric Ophthalmology/Strabismus |
|
|||
o Refractive Surgery |
|
o Retina and Vitreous Disease |
o Other: _______________________ |
|
||
|
|
|
|
|
|
|
Section B (for CCOA applicants only) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Supervisor's Name |
First |
|
|
M.I. |
Last |
|
|
|
|
|
|
|
|
Company Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
Main Company Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
Product or Service Provided |
|
|
|
Supervisor’s |
|
|
Applicant’s Job Title
8. Sponsor/Employer Endorsement
SPONSORING OPHTHAlMOlOGIST eNDORSeMeNT (for COA, COT, COMT, OSA, ROUB, CDOS applicants only)
Please check ONE of the following: o The applicant works under my direct supervision. o The applicant has my sponsorship.
(The sponsoring ophthalmologist (or physician for ROUB or CDOS) attests that he/she knows the individual applicant, certiies that the individual is knowledgeable and skilled in the ield, and that the individual is working within established JCAHPO guidelines for ophthalmic medical personnel.)
I am an ophthalmologist (or physician for ROUB or CDOS), licensed to practice medicine in:_____________________________________________________________
|
|
|
State or Province |
My license number |
|
X |
|
|
|
|
|
Sponsor’s Signature |
|
|
|
Date |
|
|
|
|
|
|
|
Sponsor's Name |
First |
|
M.I. |
Last |
|
|
|
|
|
|
|
Clinic Name |
|
|
|
|
|
|
|
|
|
|
|
Clinic Address |
|
City |
State |
Zip |
Country |
|
|
|
|
|
|
Telephone |
|
|
FAX |
|
|
eMPlOYeR’S eNDORSeMeNT (CCOA applicants only)
The employer/supervisor attests that he/she knows the individual applicant, certiies that the individual is knowledgeable and skilled in the ield, and that the
individual is working within established JCAHPO guidelines.
X
Employer’s Signature |
Date |
37
JCAHPO Application for Examination
9. Release of Examination Data
JCAHPO reserves the right to use, for any purpose, all examination data in aggregate reports related to exam performance. Release of such data will not include names or personal, identiiable information. Examples of the purposed, for which such data might be used include, but are not limited to: JCAHPO research
projects, grants, and formal training program reports.
Information regarding whether or not you are actively certiied is public and may be veriied or accessed by anyone.
If you wish to authorize JCAHPO’s release of your individual, identiiable data (name) to any source, please contact JCAHPO, in writing, with the name of the intended recipient and the time period in which release can be made.
Compliance with the Americans with Disabilities Act (ADA)
In compliance with the ADA, JCAHPO will provide reasonable accommodations for candidates with disabilities who cannot take the examination under the usual testing conditions. Disabled individuals must provide notice and appropriate documentation (at the applicant’s expense) of their disability when applying for the examination.
If accommodations are necessary for you to complete a JCAHPO examination due to functional limitations imposed by a disability, you will be required to complete and return a questionnaire. Questionnaires must be submitted with proper documentation and included with the examination application.
Application Checklist
Before mailing your application, please be sure that the following have been included:
oA copy of documentation showing successful completion of a formal educational training program or independent study course, if applicable.
oA copy of veriication of college credits or JCAHPO continuing education credits, if applicable.
oOSA applicants only: A copy of a document showing oficial accreditation of the surgical facility by a
SA2 eligibility pathway.
oCompletion of the appropriate eligibility criteria box, question #9 on section 6, and your signature on application pages 1 and 2.
oCOA, COT, COMT, OSA, ROUB, and CDOS applicants: Your sponsor’s signature (application page 3 of 4). Your sponsor must be an ophthalmologist If you
are applying for the COA, COT, COMT, or OSA exam. ROUB and CDOS applicants may have any physician serve as their sponsor. Original signatures are required - signature stamps or computerized digitized signatures are not accepted.
oCOT or COMT applicants: If using the T4 or TG5 eligibility pathway, veriication of
oCCOA applicants only: Your supervisor’s signature (application page 3 of 4). Original signatures are required - signature stamps or computerized digitized signatures are not accepted.
oCDOS applicants only: Case log of 10 abnormal ophthalmic
oExamination fee, payable to JCAHPO in U.S. dollars. (Refer to fee schedule). All applications denied due to not meeting the eligibility requirements or incomplete applications, will not receive a refund of the exam fee.
NOTe: Please retain a photocopy of your application. If any of the
incomplete, your application will not be processed. Mail (DO NOT FAX) your application to:
JCAHPO
2025 Woodlane Drive
St. Paul, MN
Once your application is accepted, you will be assigned a
will be provided to you in a conirmation letter you will receive after your application is accepted.
38