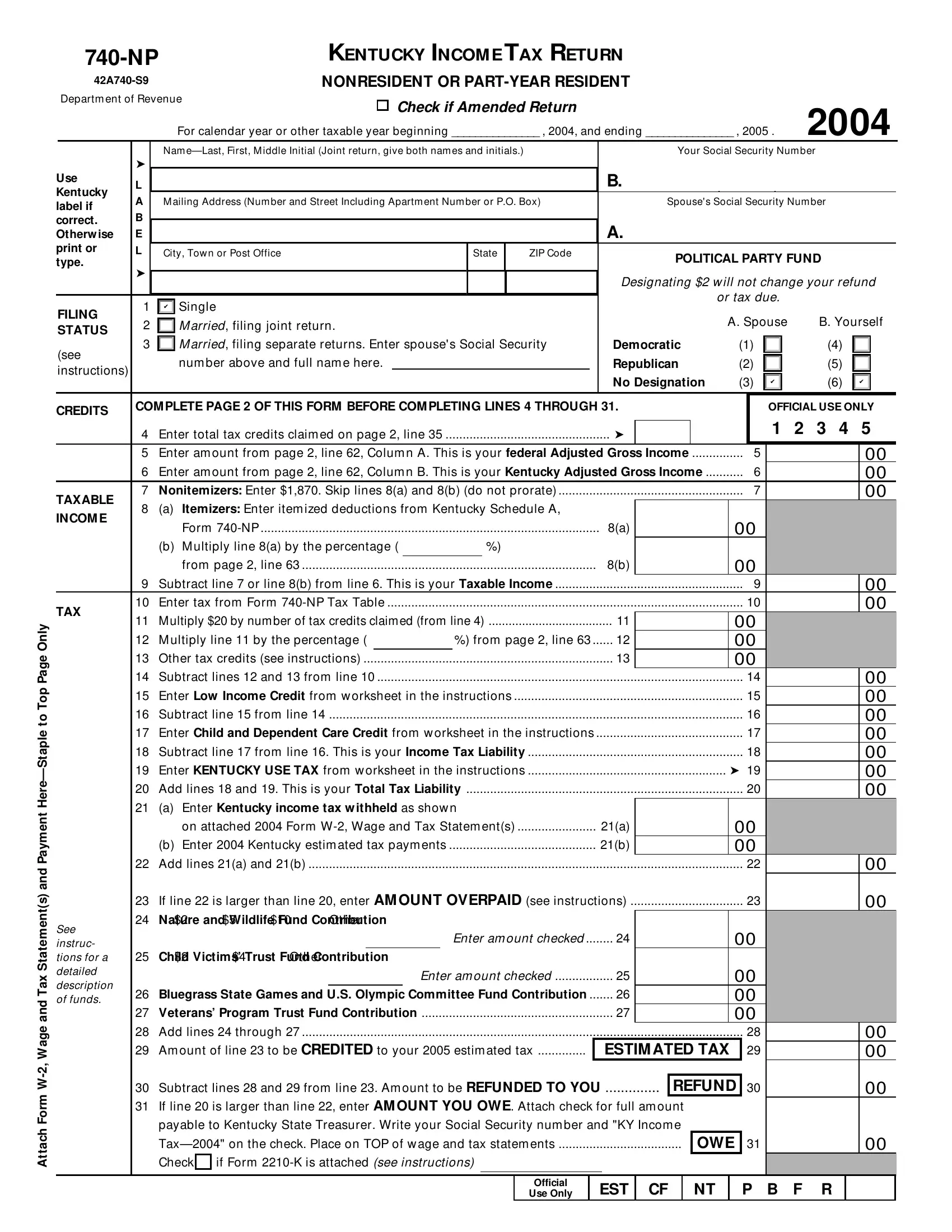
The Kentucky 740 NP form plays a crucial role for nonresidents or part-year residents as they navigate the complexities of state income tax obligations. This comprehensive document ensures that individuals who have earned income in Kentucky but do not reside there for the entire year can accurately report their earnings and calculate their tax liabilities. It accommodates various financial scenarios by requiring attachments like Form W-2, Wage and Tax Statement(s), and detailing instructions for amended returns. The form meticulously breaks down into sections covering filing status, income, tax credits, and contributions to various funds, reflecting a commitment to both taxpayer duty and community support through optional donations to causes such as child victims’ trust funds and veterans’ programs. Furthermore, distinctions between nonitemizers and itemizers, alongside specific deductions and adjustments to income, illustrate the form's adaptability to diverse financial profiles. Correctly navigating the 740 NP ensures that taxpayers meet their obligations while potentially taking advantage of credits and deductions appropriate for their filing status, thereby underscoring the importance of understanding and accurately completing this document.
| Question | Answer |
|---|---|
| Form Name | Kentucky Form 740 Np |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 42a740np itemizers enter itemized deductions from kentucky schedule a form 740 np |
Attach Form
|
|
KENTUCKY INCOM E TAX RETURN |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||
|
|
|
|
NONRESIDENT OR |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
Departm ent of Revenue |
|
|
|
|
¸ Check if Amended Return |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2004 |
|||||||||||||||||
|
|
|
|
For calendar year or other taxable year beginning _______________ , 2004, and ending _______________ , 2005 . |
|
||||||||||||||||||||||||||||||||||
|
|
|
Nam |
|
|
|
|
|
|
|
Your Social Security Num ber |
|
|
|
|
|
|||||||||||||||||||||||
Use |
➤ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
B. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
L |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Kentucky |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
A |
|
M ailing Address (Num ber and Street Including Apartm ent Num ber or P.O. Box) |
|
|
|
Spouse's Social Security Num ber |
|
|
|
|
|
||||||||||||||||||||||||||||
label if |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
correct. |
B |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Otherw ise |
E |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
print or |
L |
|
City, Tow n or Post Office |
|
|
|
State |
|
ZIP Code |
|
|
|
|
POLITICAL PARTY FUND |
|
|
|
|
|
||||||||||||||||||||
type. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
➤ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Designating $2 w ill not change your refund |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or tax due. |
|
|
|
|
|
|
|
||||||
|
1 |
|
|
Single |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
✔ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
FILING |
2 |
|
|
M arried, filing joint return. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. Spouse |
|
B. Yourself |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
STATUS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
3 |
|
|
M arried, filing separate returns. Enter spouse's Social Security |
Democratic |
(1) |
|
|
|
|
|
(4) |
|
|
|
|
||||||||||||||||||||||||
(see |
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||
|
|
|
num ber above and full nam e here. |
|
|
|
|
|
|
|
|
|
Republican |
(2) |
|
|
|
|
|
(5) |
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
instructions) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No Designation |
(3) |
|
|
|
|
|
(6) |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
✔ |
|
|
|
|
✔ |
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
CREDITS |
COM PLETE PAGE 2 OF THIS FORM BEFORE COM PLETING LINES 4 THROUGH 31. |
|
|
|
|
OFFICIAL USE ONLY |
|||||||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
Enter total tax credits claim ed on page 2, line 35 |
|
|
➤ |
|
|
|
|
|
|
|
|
|
1 |
|
2 |
3 |
4 |
|
5 |
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
5 |
|
Enter am ount from page 2, line 62, Colum n A. This is your federal Adjusted Gross Income |
5 |
|
|
|
|
|
|
|
00 |
|||||||||||||||||||||||||||
|
6 |
|
Enter am ount from page 2, line 62, Colum n B. This is your Kentucky Adjusted Gross Income |
6 |
|
|
|
|
|
|
|
00 |
|||||||||||||||||||||||||||
TAXABLE |
7 |
|
Nonitemizers: Enter $1,870. Skip lines 8(a) and 8(b) (do not prorate) |
|
|
|
|
|
7 |
|
|
|
|
|
|
|
00 |
||||||||||||||||||||||
INCOM E |
8 |
|
(a) |
Itemizers: Enter item ized deductions from Kentucky Schedule A, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
Form |
|
|
|
|
|
|
|
|
|
8(a) |
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
(b) |
M ultiply line 8(a) by the percentage ( |
%) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
from page 2, line 63 |
|
|
|
|
|
|
|
|
8(b) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
9 |
|
Subtract line 7 or line 8(b) from line 6. This is your Taxable Income |
|
|
|
|
|
9 |
|
|
|
|
|
|
|
00 |
||||||||||||||||||||||
TAX |
10 |
|
Enter tax from Form |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
00 |
|||||||||||||
11 |
|
M ultiply $20 by num ber of tax credits claim ed (from line 4) |
|
|
11 |
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
12 |
|
M ultiply line 11 by the percentage ( |
|
|
|
%) from page 2, line 63 |
12 |
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
13 |
|
Other tax credits (see instructions) |
|
|
|
|
|
|
|
|
13 |
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
14 |
|
Subtract lines 12 and 13 from line 10 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14 |
|
|
|
|
|
|
|
00 |
|||||||||||||
|
15 |
|
Enter Low Income Credit from w orksheet in the instructions |
|
|
|
|
|
|
|
|
15 |
|
|
|
|
|
|
|
00 |
|||||||||||||||||||
|
16 |
|
Subtract line 15 from line 14 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
16 |
|
|
|
|
|
|
|
00 |
|||||||||||||
|
17 |
|
Enter Child and Dependent Care Credit from w orksheet in the instructions |
|
|
|
|
|
17 |
|
|
|
|
|
|
|
00 |
||||||||||||||||||||||
|
18 |
|
Subtract line 17 from line 16. This is your Income Tax Liability |
|
|
|
|
|
|
|
|
18 |
|
|
|
|
|
|
|
00 |
|||||||||||||||||||
|
19 |
|
Enter KENTUCKY USE TAX from w orksheet in the instructions |
|
|
|
|
|
|
|
|
➤ 19 |
|
|
|
|
|
|
00 |
||||||||||||||||||||
|
20 |
|
Add lines 18 and 19. This is your Total Tax Liability |
|
|
|
|
|
|
|
|
20 |
|
|
|
|
|
|
|
00 |
|||||||||||||||||||
|
21 |
|
(a) |
Enter Kentucky income tax w ithheld as show n |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
on attached 2004 Form |
|
|
21(a) |
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
(b) |
Enter 2004 Kentucky estim ated tax paym ents |
|
|
21(b) |
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
22 |
|
Add lines 21(a) and 21(b) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22 |
|
|
|
|
|
|
|
00 |
|||||||||||||
|
23 |
|
.................................If line 22 is larger than line 20, enter AM OUNT OVERPAID (see instructions) |
23 |
|
|
|
|
|
|
|
00 |
|||||||||||||||||||||||||||
See |
24 Nature and Wildlife Fund Contribution |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
¸ $2 |
¸ $5 |
¸ $10 ¸ Other |
|
|
|
Enter am ount checked |
24 |
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
instruc- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
tions for a |
25 |
|
Child Victims’ Trust Fund Contribution |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
detailed |
|
¸ $2 |
¸ $4 |
¸ Other |
|
|
Enter am ount checked |
25 |
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
description |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
26 |
|
Bluegrass State Games and U.S. Olympic Committee Fund Contribution |
26 |
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
of funds. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||
|
27 |
|
Veterans’ Program Trust Fund Contribution |
........................................................ |
|
|
|
|
|
|
|
27 |
|
|
|
|
|
00 |
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
28 |
|
Add lines 24 through 27 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
28 |
|
|
|
|
|
|
|
00 |
||||||||||||
|
29 |
|
..............Am ount of line 23 to be CREDITED to your 2005 estim ated tax |
|
ESTIM ATED TAX |
|
29 |
|
|
|
|
|
|
|
00 |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
30 |
|
Subtract lines 28 and 29 from line 23. Am ount to be REFUNDED TO YOU |
.............. |
|
|
REFUND |
30 |
|
|
|
|
|
|
|
00 |
|||||||||||||||||||||||
31If line 20 is larger than line 22, enter AM OUNT YOU OWE. Attach check for full am ount payable to Kentucky State Treasurer. Write your Social Security num ber and "KY Incom e
OWE 31 |
00 |
|
Check ¸ if Form |
|
|
Official |
|
|
Use Only |
EST CF NT P B F |
R |