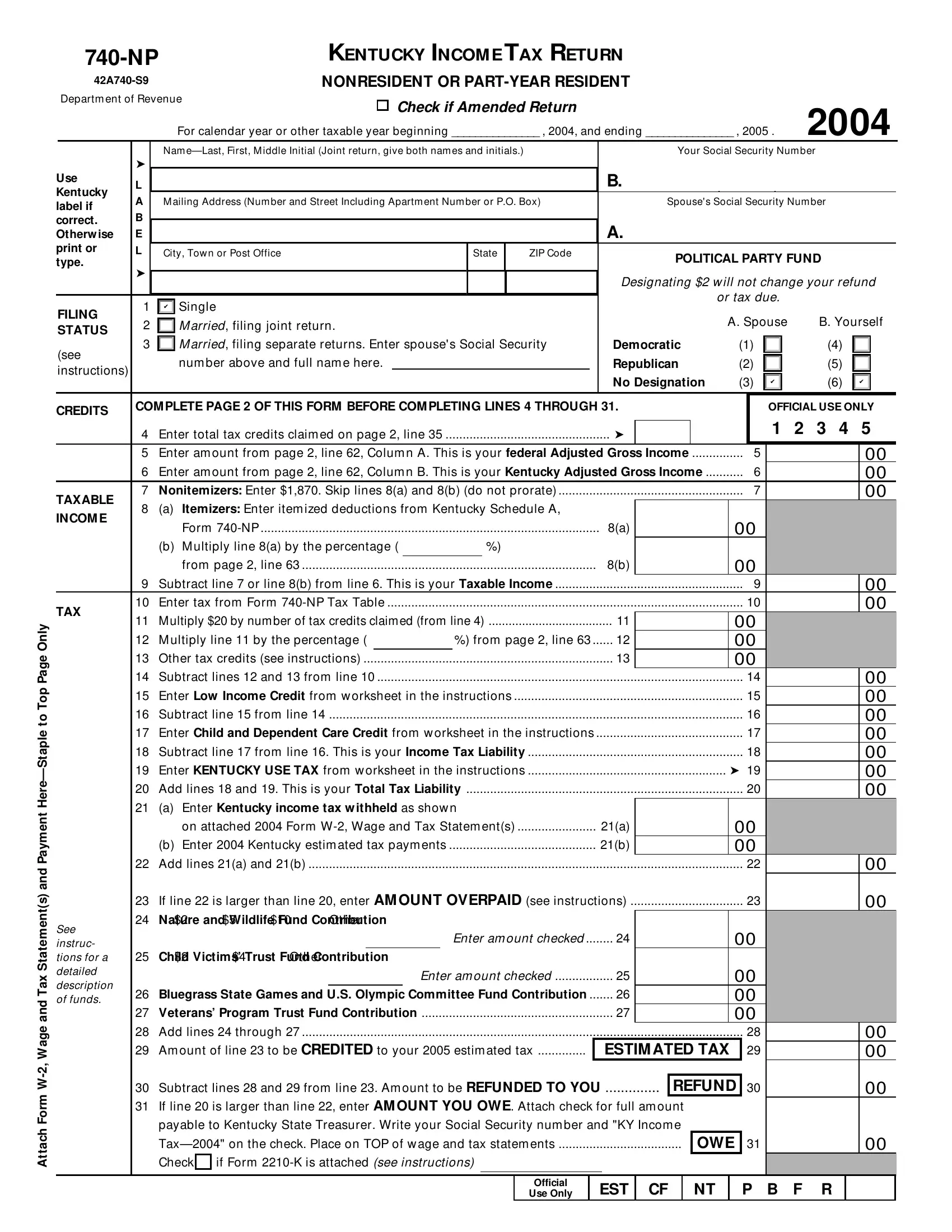
The Kentucky 740 NP form plays a crucial role for nonresidents or part-year residents as they navigate the complexities of state income tax obligations. This comprehensive document ensures that individuals who have earned income in Kentucky but do not reside there for the entire year can accurately report their earnings and calculate their tax liabilities. It accommodates various financial scenarios by requiring attachments like Form W-2, Wage and Tax Statement(s), and detailing instructions for amended returns. The form meticulously breaks down into sections covering filing status, income, tax credits, and contributions to various funds, reflecting a commitment to both taxpayer duty and community support through optional donations to causes such as child victims’ trust funds and veterans’ programs. Furthermore, distinctions between nonitemizers and itemizers, alongside specific deductions and adjustments to income, illustrate the form's adaptability to diverse financial profiles. Correctly navigating the 740 NP ensures that taxpayers meet their obligations while potentially taking advantage of credits and deductions appropriate for their filing status, thereby underscoring the importance of understanding and accurately completing this document.
| Question | Answer |
|---|---|
| Form Name | Kentucky Form 740 Np |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | 42a740np itemizers enter itemized deductions from kentucky schedule a form 740 np |