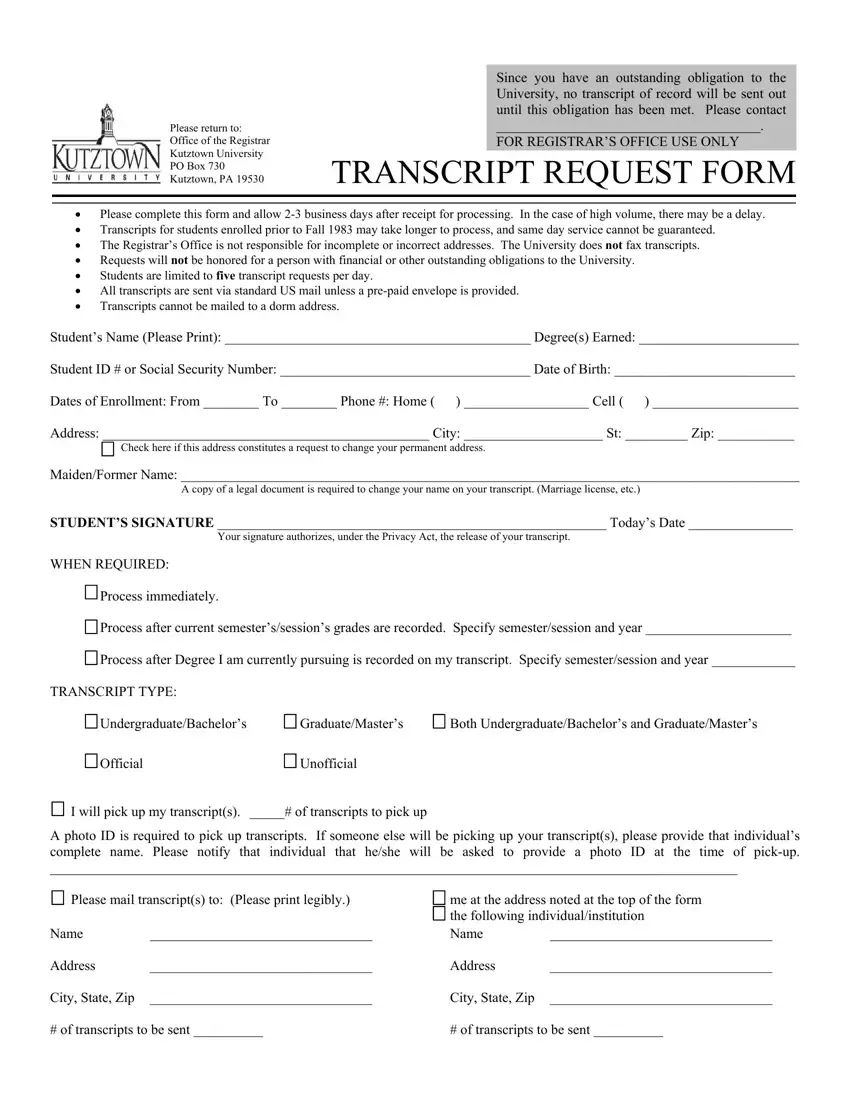
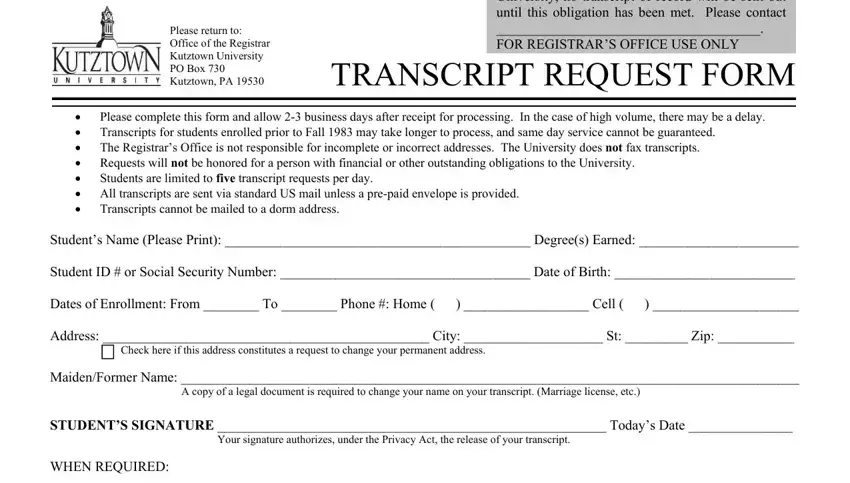
Please complete this form and allow 2-3 business days after receipt for processing. In the case of high volume, there may be a delay.
Transcripts for students enrolled prior to Fall 1983 may take longer to process, and same day service cannot be guaranteed.
The Registrar’s Office is not responsible for incomplete or incorrect addresses. The University does NOT fax transcripts.
Requests will NOT be honored for a person with financial or other outstanding obligations to the University.
Students are limited to FIVE transcript requests per day.
All transcripts are sent via standard US mail unless a pre-paid envelope is provided.
Transcripts cannot be mailed to a dorm address.
Student’s Name (Please Print): ____________________________________________ Degree(s) Earned: _______________________
Student ID # or Social Security Number: ____________________________________ Date of Birth: __________________________
Dates of Enrollment: From ________ To ________ Phone #: Home ( ) __________________ Cell ( ) _____________________
Address: _______________________________________________ City: ____________________ St: _________ Zip: ___________
 Check here if this address constitutes a request to change your permanent address.
Check here if this address constitutes a request to change your permanent address.
Maiden/Former Name: _________________________________________________________________________________________
A copy of a legal document is required to change your name on your transcript. (Marriage license, etc.)
STUDENT’S SIGNATURE ________________________________________________________ Today’s Date _______________
Your signature authorizes, under the Privacy Act, the release of your transcript.
WHEN REQUIRED:
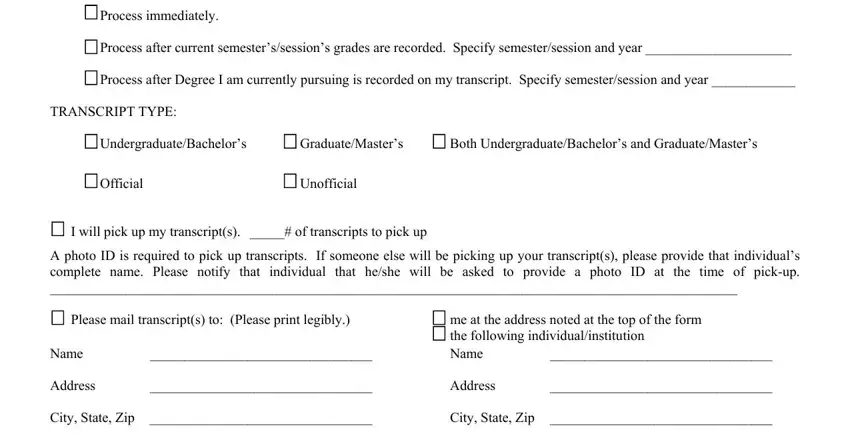
 Process immediately.
Process immediately.
 Process after current semester’s/session’s grades are recorded. Specify semester/session and year _____________________
Process after current semester’s/session’s grades are recorded. Specify semester/session and year _____________________
 Process after Degree I am currently pursuing is recorded on my transcript. Specify semester/session and year ____________
Process after Degree I am currently pursuing is recorded on my transcript. Specify semester/session and year ____________
TRANSCRIPT TYPE: |
|
|
Undergraduate/Bachelor’s |
Graduate/Master’s |
Both Undergraduate/Bachelor’s and Graduate/Master’s |
Official |
Unofficial |
|
 I will pick up my transcript(s). _____# of transcripts to pick up
I will pick up my transcript(s). _____# of transcripts to pick up
A photo ID is required to pick up transcripts. If someone else will be picking up your transcript(s), please provide that individual’s complete name. Please notify that individual that he/she will be asked to provide a photo ID at the time of pick-up.
___________________________________________________________________________________________________
Please mail transcript(s) to: (Please print legibly.) |
me at the address noted at the top of the form |
|
|
the following individual/institution |
Name |
________________________________ |
Name |
________________________________ |
Address |
________________________________ |
Address |
________________________________ |
City, State, Zip |
________________________________ |
City, State, Zip |
________________________________ |
# of transcripts to be sent __________ |
# of transcripts to be sent __________ |