
When you need to fill out db450, it's not necessary to install any applications - just try our online PDF editor. To maintain our editor on the forefront of practicality, we aim to integrate user-oriented features and improvements regularly. We're routinely pleased to get feedback - help us with reshaping PDF editing. It merely requires several basic steps:
Step 1: Click the "Get Form" button above on this page to get into our tool.
Step 2: As soon as you start the PDF editor, you will find the document made ready to be completed. In addition to filling in various blanks, you may also perform many other actions with the form, including adding custom words, modifying the original textual content, adding graphics, affixing your signature to the document, and more.
As for the blanks of this precise PDF, this is what you want to do:
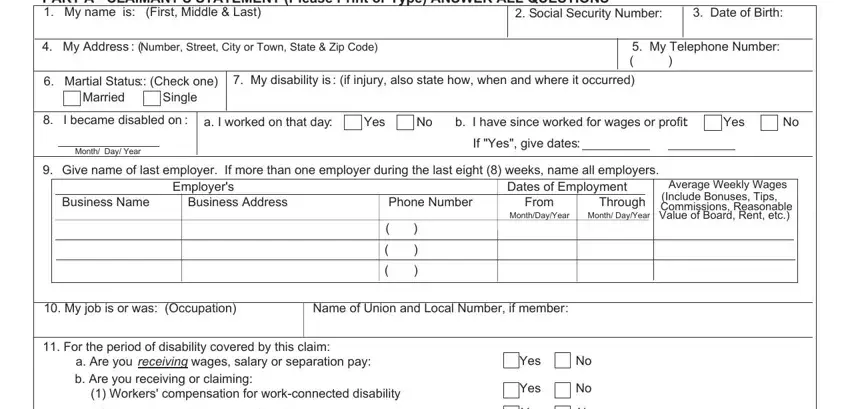
1. It is very important complete the db450 accurately, hence be mindful while filling in the sections including all these blanks:
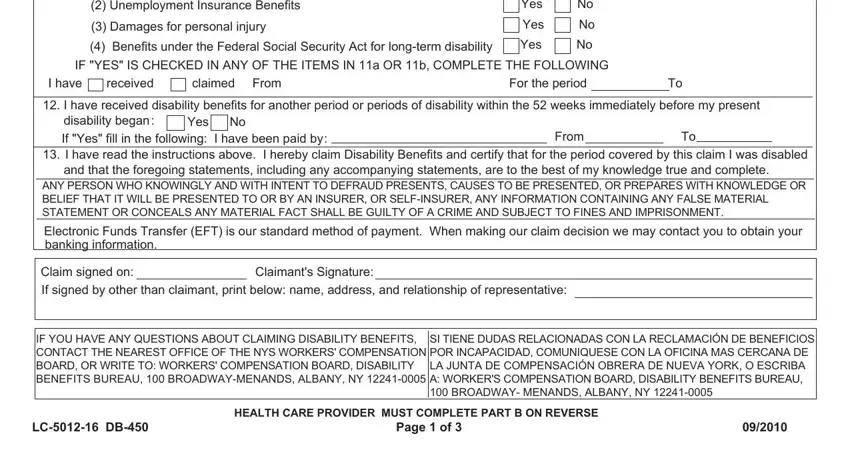
2. Just after filling out the previous part, go to the next part and complete all required details in these blanks - a Are you receiving wages salary, Workers compensation for, Yes No Yes No Yes No Yes No, IF YES IS CHECKED IN ANY OF THE, I have received claimed I have, From, For the period, If Yes fill in the following I, From To, I have read the instructions, Claim signed on If signed by other, Claimants Signature, IF YOU HAVE ANY QUESTIONS ABOUT, SI TIENE DUDAS RELACIONADAS CON LA, and LC DB.
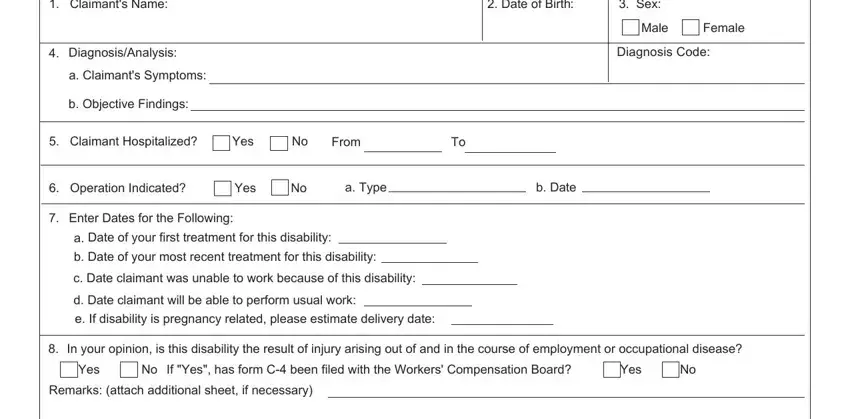
3. In this specific part, have a look at Claimants Name, Date of Birth, Sex, DiagnosisAnalysis a Claimants, b Objective Findings, Claimant Hospitalized Yes No, From To, Male Female, Diagnosis Code, Operation Indicated Yes No, a Type, b Date, Enter Dates for the Following, Date of your first treatment for, and b Date of your most recent. All these need to be taken care of with highest accuracy.
4. The following section comes with all of the following fields to consider: I affirm that I am a, Chiropractor, Physician Psychologist, Dentist, Podiatrist, NurseMidwife, License Number, Licensed in the State of, ANY PERSON WHO KNOWINGLY AND WITH, Health Care Providers Signature, Date, Health Care Providers Name Please, Office Address Number Street City, Telephone Number, and HIPAA NOTICE In order to.
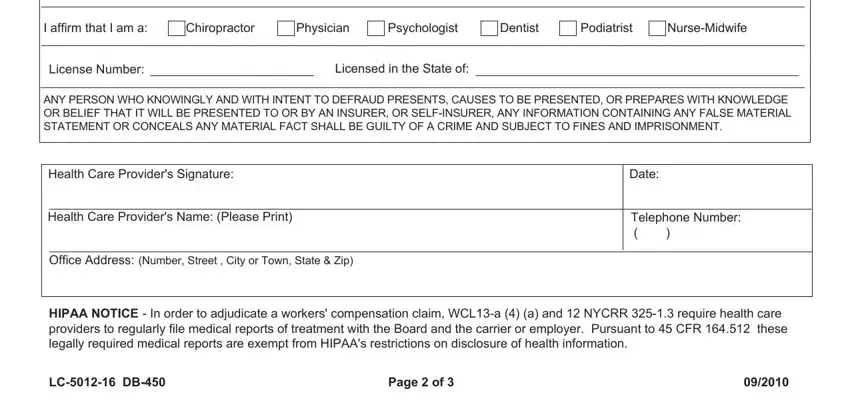
Be very mindful when filling in Health Care Providers Name Please and Date, because this is the part in which a lot of people make some mistakes.
5. As a final point, the following final segment is what you will need to complete before using the form. The blanks in this case include the following: PART C EMPLOYERS STATEMENT, Social Securit y Number, Employees Address Street City, Date of Birth, Date of employment, Full Time, Part Time, Check days normally worked, Sun Mon Tues Wed Thurs Fri Sat, If Part Time give particulars, s employee a Union member I, Yes No, If Yes is employee entitled to, Occupation, and Yes No.
Step 3: Make sure that your details are correct and then just click "Done" to continue further. After getting afree trial account here, you'll be able to download db450 or email it without delay. The PDF document will also be easily accessible via your personal account with all of your modifications. With FormsPal, you're able to fill out documents without being concerned about personal information incidents or records getting shared. Our protected platform ensures that your personal information is kept safe.