
Through the online PDF tool by FormsPal, it is possible to complete or alter change right here and now. The editor is consistently maintained by our team, receiving handy features and turning out to be better. It just takes a couple of simple steps:
Step 1: Access the PDF file inside our tool by hitting the "Get Form Button" at the top of this webpage.
Step 2: As soon as you access the PDF editor, you will see the document all set to be filled out. Aside from filling out various blanks, you may also do many other things with the file, such as adding your own textual content, changing the initial textual content, inserting graphics, signing the form, and a lot more.
This PDF form will require particular information to be typed in, therefore you should definitely take some time to enter what's asked:
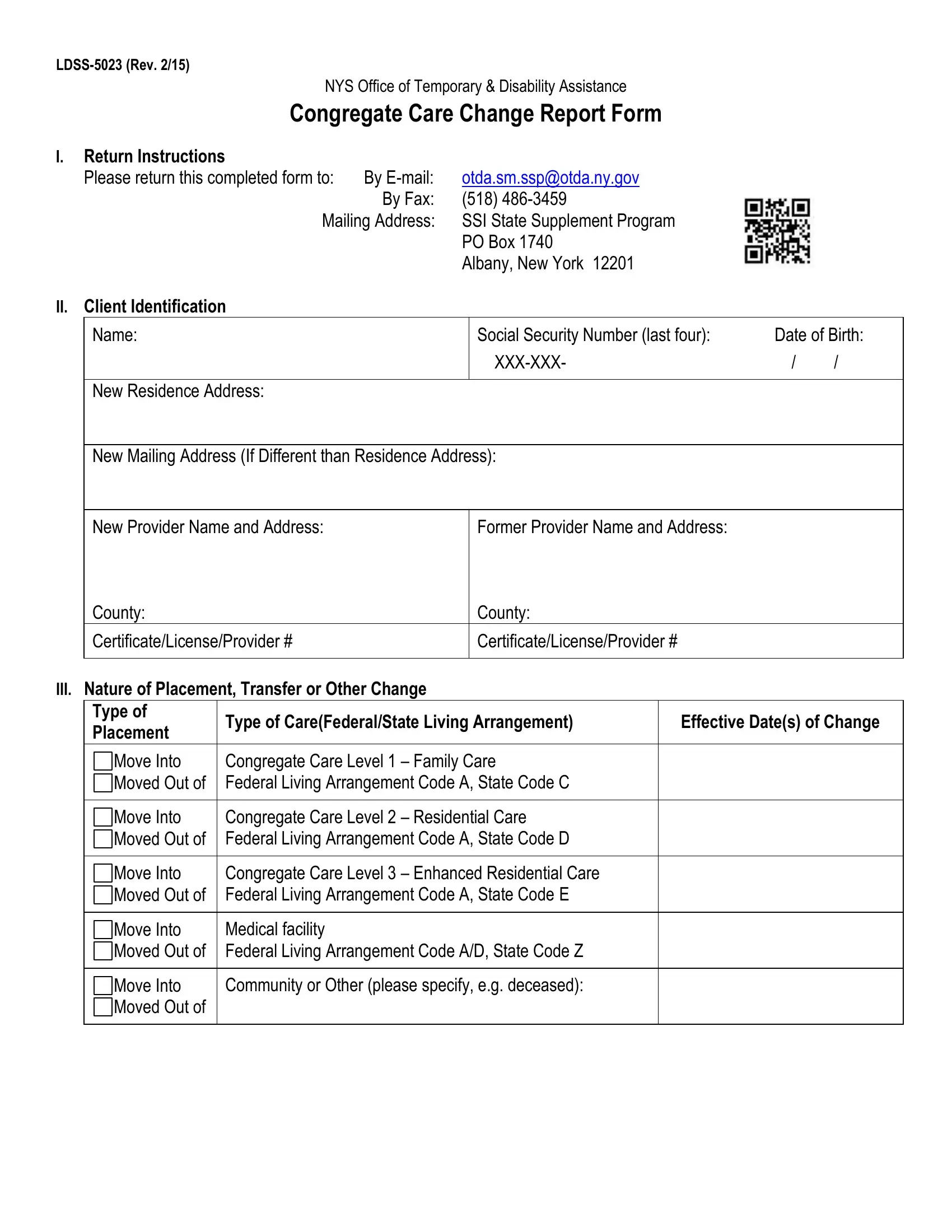
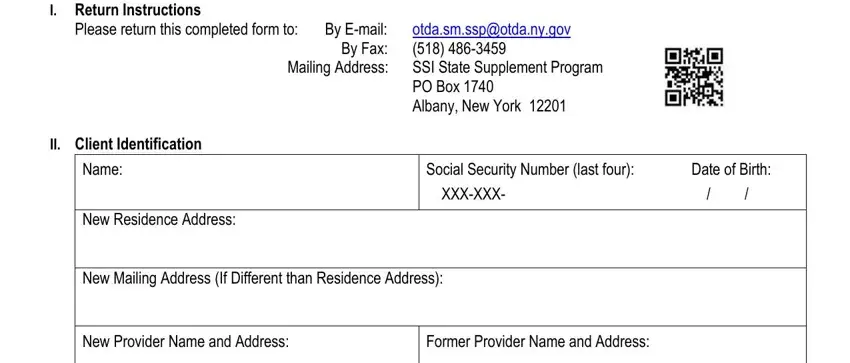
1. The change needs certain details to be entered. Be sure that the subsequent fields are finalized:
2. Once the previous array of fields is done, you're ready insert the necessary specifics in Have Questions or need More, and wwwotdanygovprogramsssp in order to progress to the next step.

It's easy to make errors when completing your Have Questions or need More, consequently make sure you look again before you finalize the form.
Step 3: Spell-check all the details you've inserted in the blank fields and then click the "Done" button. Get hold of the change as soon as you sign up for a free trial. Conveniently gain access to the pdf file within your personal account, along with any modifications and changes being all synced! At FormsPal.com, we endeavor to make sure all of your details are maintained protected.