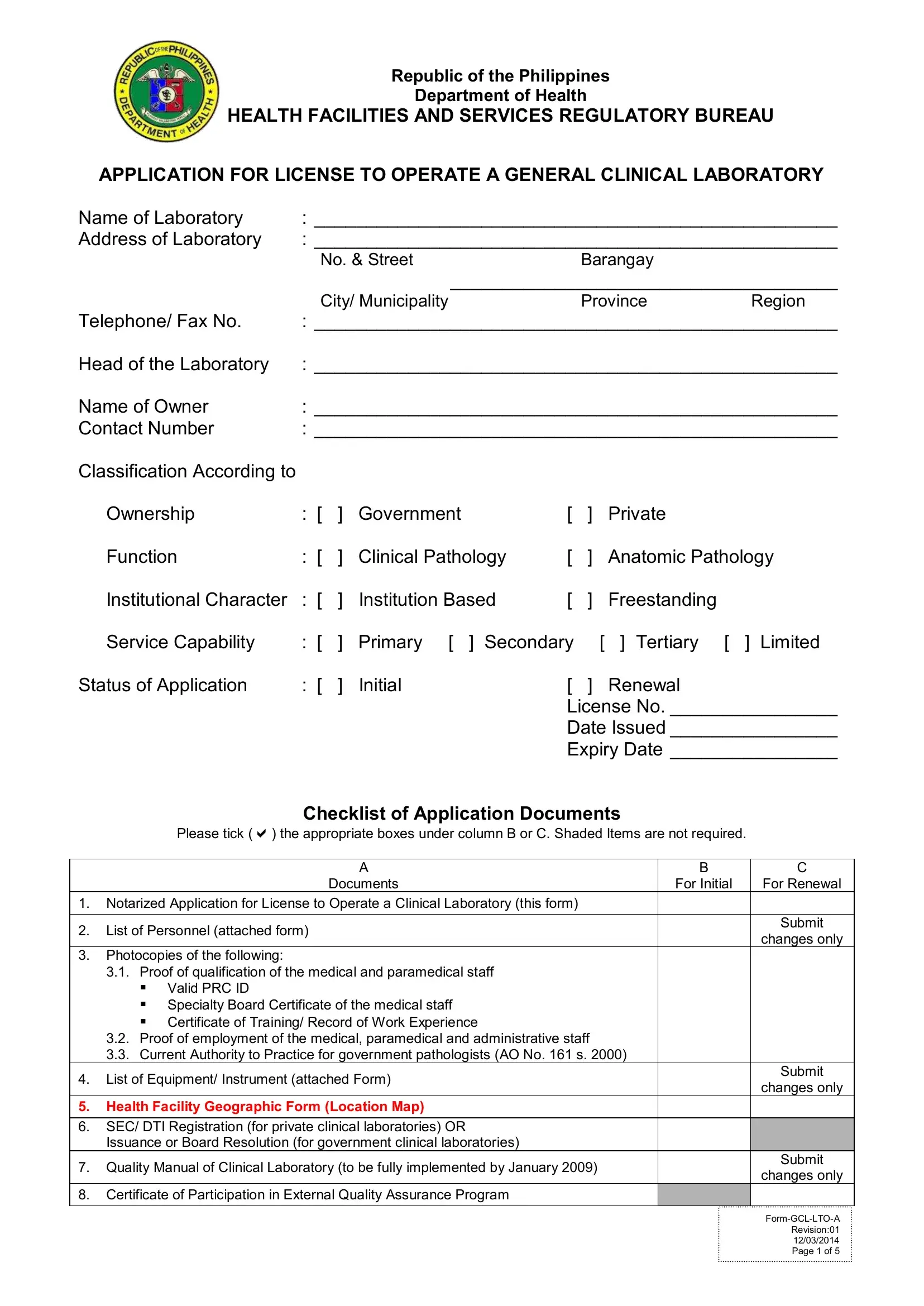
In the pursuit of maintaining high standards for health facilities, the Republic of the Philippines Department of Health stipulates a thorough application process for the licensing of general clinical laboratories. This process, detailed in the License to Operate Clinical Laboratory DPH form, is comprehensive, requiring laboratories to present a broad spectrum of documentation and evidence of compliance with the country's health regulations. Laboratories must provide notarized applications, detailed lists of personnel, qualifications of staff, proof of employment, equipment inventories, and even geographic information about the facility's location. For both government and private institutions aiming to offer clinical or anatomic pathology services, this form serves as the starting point. It is meticulous in its demand for information on the laboratory's ownership, function, institutional character, and service capability, whether applying for an initial license or renewing an existing one. Additionally, laboratories must adhere to quality standards by submitting a quality manual, proof of participation in external quality assurance programs, and the credentials of the head of the laboratory, ensuring that operations align with Administrative Order No. 2007-0027, "Revised Rules and Regulations Governing the Licensure and Regulation of Clinical Laboratories in the Philippines."
| Question | Answer |
|---|---|
| Form Name | License To Operate Clinical Laboratory Dph Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | renewal of clinical laboratory license, doh license to operate, doh application form for renewal of license to operate 2021, doh application for license to operate a clinical laboratory 2019 |

Republic of the Philippines
Department of Health
HEALTH FACILITIES AND SERVICES REGULATORY BUREAU
APPLICATION FOR LICENSE TO OPERATE A GENERAL CLINICAL LABORATORY
Name of Laboratory |
: __________________________________________________ |
|||||||||
Address of Laboratory |
: __________________________________________________ |
|||||||||
|
|
No. & Street |
|
Barangay |
|
|
||||
|
|
|
|
_____________________________________ |
||||||
|
|
City/ Municipality |
|
Province |
Region |
|||||
Telephone/ Fax No. |
: __________________________________________________ |
|||||||||
Head of the Laboratory |
: __________________________________________________ |
|||||||||
Name of Owner |
: __________________________________________________ |
|||||||||
Contact Number |
: __________________________________________________ |
|||||||||
Classification According to |
|
|
|
|
|
|
|
|
|
|
|
Ownership |
: [ |
] |
Government |
[ |
] |
Private |
|
|
|
|
Function |
: [ |
] |
Clinical Pathology |
[ |
] |
Anatomic Pathology |
|||
|
Institutional Character |
: [ |
] |
Institution Based |
[ |
] |
Freestanding |
|
|
|
|
Service Capability |
: [ |
] |
Primary [ ] Secondary |
[ |
] Tertiary [ ] |
|
Limited |
||
Status of Application |
: [ |
] |
Initial |
[ |
] |
Renewal |
|
|
||
|
|
|
|
|
License No. ________________ |
|||||
|
|
|
|
|
Date Issued ________________ |
|||||
|
|
|
|
|
Expiry Date ________________ |
|||||
|
|
Checklist of Application Documents |
|
|
||||||
|
Please tick () the appropriate boxes under column B or C. Shaded Items are not required. |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A |
|
|
|
B |
|
C |
|
|
|
Documents |
|
|
|
For Initial |
|
For Renewal |
|
1. |
Notarized Application for License to Operate a Clinical Laboratory (this form) |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
2. |
List of Personnel (attached form) |
|
|
|
|
|
|
|
Submit |
|
|
|
|
|
|
|
|
changes only |
|||
|
|
|
|
|
|
|
|
|
|
|
3. Photocopies of the following: |
|
|
|
|
|
|
|
|
|
|
|
3.1. Proof of qualification of the medical and paramedical staff |
|
|
|
|
|
|
|||
|
▪ Valid PRC ID |
|
|
|
|
|
|
|
|
|
|
▪ Specialty Board Certificate of the medical staff |
|
|
|
|
|
|
|||
|
▪ Certificate of Training/ Record of Work Experience |
|
|
|
|
|
|
|||
|
3.2. Proof of employment of the medical, paramedical and administrative staff |
|
|
|
|
|||||
|
3.3. Current Authority to Practice for government pathologists (AO No. 161 s. 2000) |
|
|
|
||||||
4. |
List of Equipment/ Instrument (attached Form) |
|
|
|
|
|
Submit |
|||
|
|
|
|
|
changes only |
|||||
|
|
|
|
|
|
|
|
|
|
|
5. Health Facility Geographic Form (Location Map) |
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|||
6. |
SEC/ DTI Registration (for private clinical laboratories) OR |
|
|
|
|
|
|
|||
|
Issuance or Board Resolution (for government clinical laboratories) |
|
|
|
|
|
|
|||
7. |
Quality Manual of Clinical Laboratory (to be fully implemented by January 2009) |
|
|
|
Submit |
|||||
|
|
|
changes only |
|||||||
|
|
|
|
|
|
|
|
|
|
|
8. |
Certificate of Participation in External Quality Assurance Program |
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Revision:01 |
|
|
|
|
|
|
|
|
|
12/03/2014 |
|
|
|
|
|
|
|
|
|
|
|
Page 1 of 5 |
Acknowledgement
REPUBLIC OF THE PHILIPPINES |
) |
|
CITY/ MUNICIPALITY OF ______________) S.S. |
|
|
I, ______________________________, ____________, |
of legal age, __________, a resident of |
|
Name |
Civil Status |
Age |
___________________________________________, after having been sworn in accordance with law hereby depose and
Address
say that I am executing this affidavit to attest to the completeness and truth of the foregoing information and the attached
documents required for the Licensure and Regulation of Clinical Laboratories in the Philippines pursuant to Administrative
Order No.
the Philippines”.
|
|
|
|
|
_________________________ |
|
|
|
|
|
Signature |
Before me, this _________day |
of ______________ 20 |
|
|
in the |
City/ Municipality of ________________, |
|
|||||
Philippines, personally appeared |
|
|
|
|
|
Owner |
Community Tax Number |
|
Issued at/ on |
||
_______________________________ |
_________________________ |
_________________________ |
|||
known to me to be the same person/s who executed the foregoing instrument and they acknowledge to me that the same is
their free act and deed.
IN WITNESS WHEREOF, I have hereunto set my hands this _________day of _______________ 20
Doc. No. ____________________ |
NOTARY PUBLIC |
Page No. ____________________ |
My Commission Expires |
Book No. ____________________ |
Dec. 31, _______ |
Series of ____________________ |
|
|
|
|
Revision:01 |
|
12/03/2014 |
|
Page 2 of 5 |
APPLICATION AS HEAD OF CLINICAL LABORATORY
The Director
Department of Health
Sir,
In compliance with the requirements of Republic Act (RA) No. 4688 and Administrative Order (AO) No.
_________________________________________
Name of Clinical Laboratory
_________________________________________
Address of Clinical Laboratory
I. Name of Applicant: _______________________________________________________
Landline No.: ________________________ Mobile No.: _______________________
Address: _______________________________________________________________
II. Education and Training (Use additional sheets if necessary):
Medical School/ Institution _____________________________________________
Inclusive Dates/ Year Graduated ________________________________________
|
Specialty Board |
|
Date Certified |
Training Institution |
PBP1 Anatomic Pathology |
|
|
||
PBP Clinical Pathology |
|
|
||
PBP |
Anatomic |
and |
|
|
Clinical Pathology |
|
|
|
|
Others: Specify |
|
|
|
|
III. List all clinical laboratories supervised/ headed or associated with:
Name and Address of Clinical Laboratory |
Working Time |
Work Schedule |
A. As Head |
|
|
B. As Associate |
|
|
I hereby certify that the foregoing statements are true. I assume full responsibility that the operation of the clinical laboratory is in accordance with the Rules and Regulations pursuant to RA 4688 and AO No.
______________________________
Signature over Printed Name
___________________
Date
1PBP – Philippine Board of Pathology
|
List of Personnel |
Annex A |
|
Name of Laboratory |
: ______________________________________________________________________________________ |
Address of Laboratory |
: ______________________________________________________________________________________ |
Name
Designation/ Position
Highest Educational
Attainment
PRC Reg. No.
Valid
From |
To |
|
|
Date of Birth
(mm/dd/yr)
Signature
Annex A- List of Personnel
Revision:01
12/03/2014
Page 4 of 5
|
List of Equipment2 |
Annex B |
|
Name of Laboratory |
: ______________________________________________________________________________________ |
Address of Laboratory |
: ______________________________________________________________________________________ |
Brand Name & Model
Serial No.
Quantity
Date of Purchase
2 Equipment shall be functional and present in the clinical laboratory applying for license to operate.
Annex B- List of Equipment
Revision:01
12/03/2014
Page 5 of 5