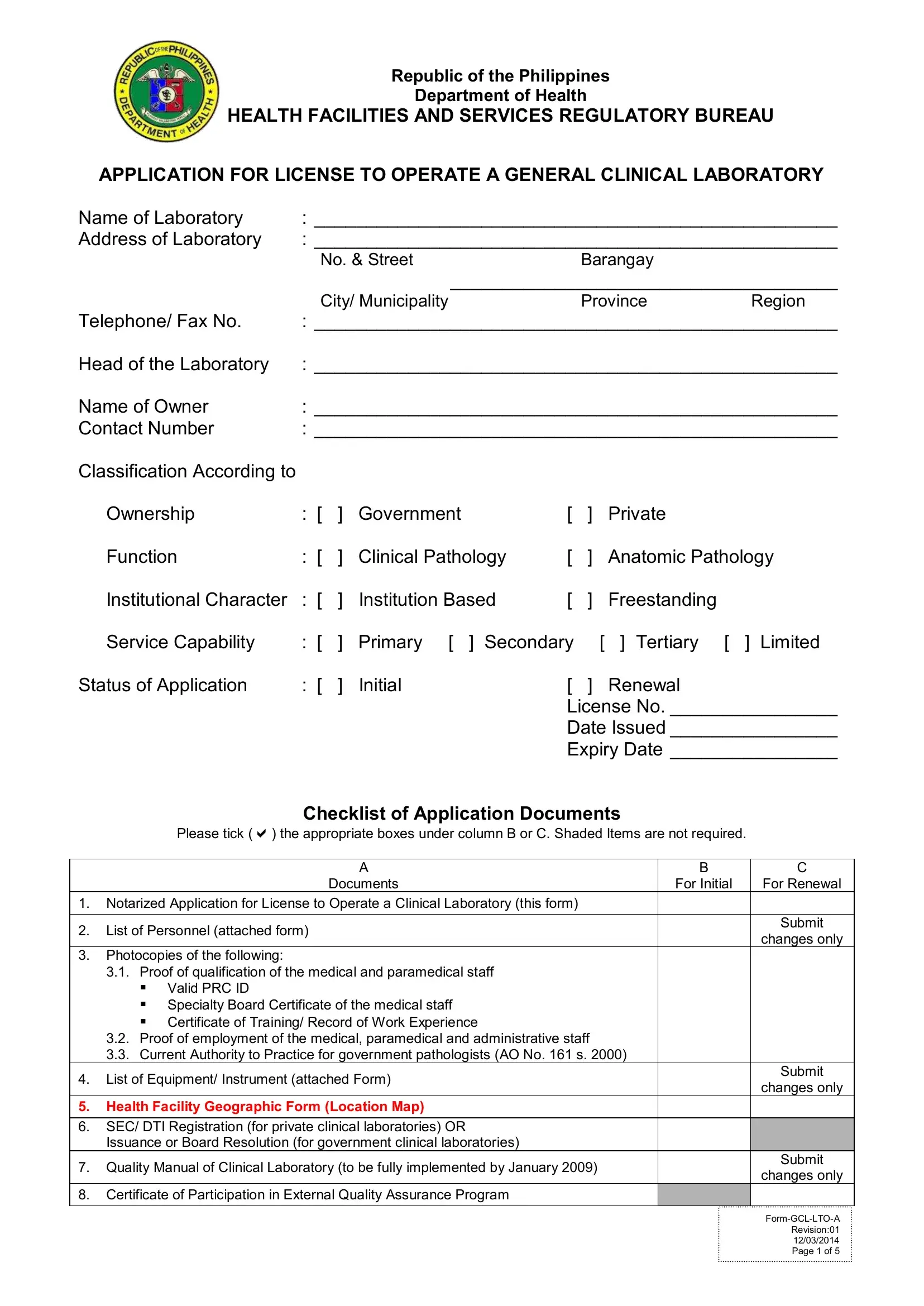
In the pursuit of maintaining high standards for health facilities, the Republic of the Philippines Department of Health stipulates a thorough application process for the licensing of general clinical laboratories. This process, detailed in the License to Operate Clinical Laboratory DPH form, is comprehensive, requiring laboratories to present a broad spectrum of documentation and evidence of compliance with the country's health regulations. Laboratories must provide notarized applications, detailed lists of personnel, qualifications of staff, proof of employment, equipment inventories, and even geographic information about the facility's location. For both government and private institutions aiming to offer clinical or anatomic pathology services, this form serves as the starting point. It is meticulous in its demand for information on the laboratory's ownership, function, institutional character, and service capability, whether applying for an initial license or renewing an existing one. Additionally, laboratories must adhere to quality standards by submitting a quality manual, proof of participation in external quality assurance programs, and the credentials of the head of the laboratory, ensuring that operations align with Administrative Order No. 2007-0027, "Revised Rules and Regulations Governing the Licensure and Regulation of Clinical Laboratories in the Philippines."
| Question | Answer |
|---|---|
| Form Name | License To Operate Clinical Laboratory Dph Form |
| Form Length | 6 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 30 sec |
| Other names | renewal of clinical laboratory license, doh license to operate, doh application form for renewal of license to operate 2021, doh application for license to operate a clinical laboratory 2019 |