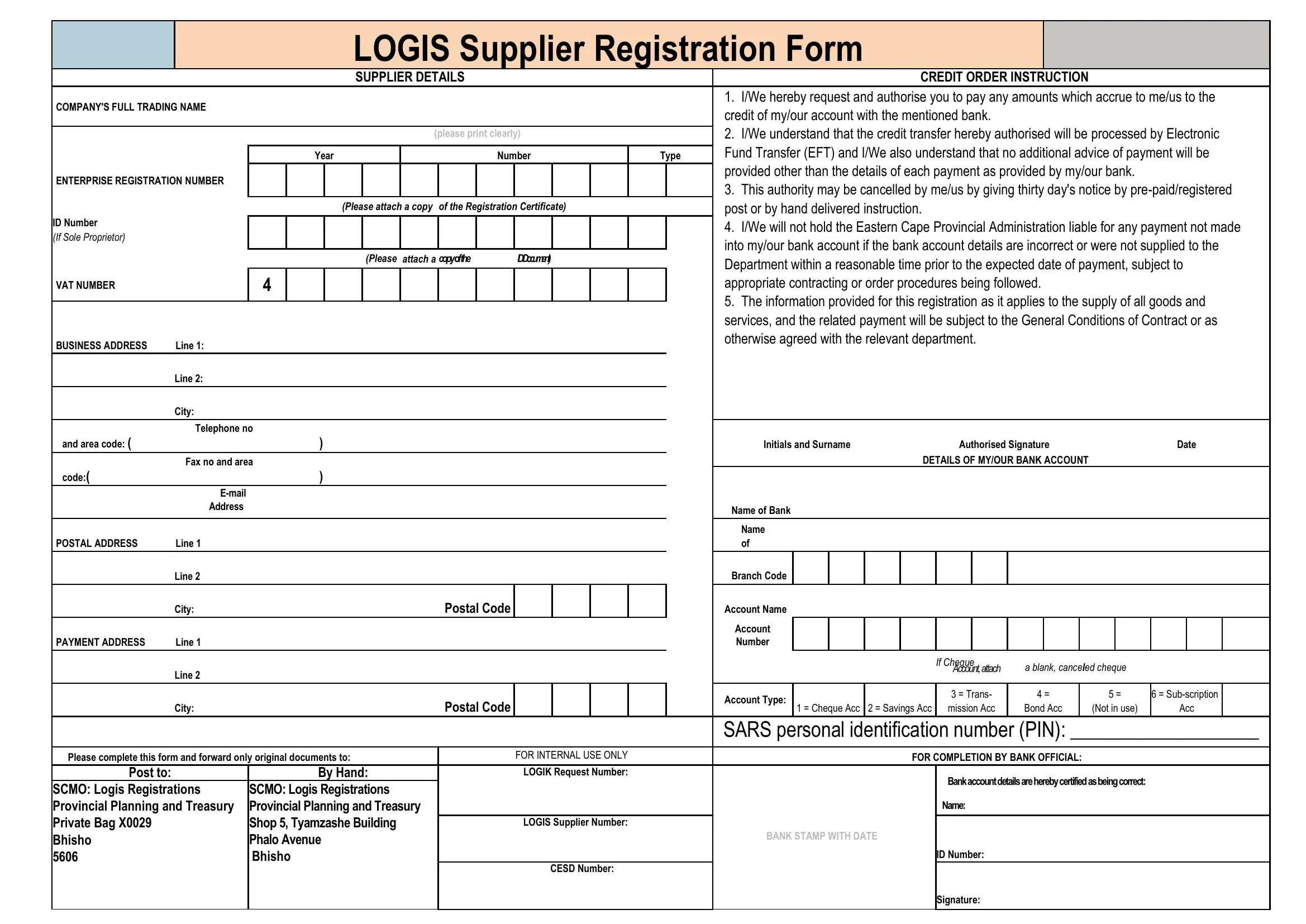
The Logis Supplier Registration Form is a critical document for suppliers looking to engage in business with entities that utilize the LOGIS system, especially within the public sector. It comprises several sections, each designed to collect comprehensive information about the supplier, ranging from the supplier's details to specific banking information necessary for electronic fund transfers (EFT). The form begins by asking for the company's full trading name and proceeds to gather essential details for executing credit order instructions, explicitly requiring the supplier to authorize payments to be credited to their account via EFT. A noteworthy aspect is the emphasis on ensuring that the supplier provides correct and complete bank account details to avoid any delays or errors in payments. Additional segments of the form collect enterprise registration numbers, VAT numbers, and personal identification details for sole proprietors, underscoring the importance of verifying the supplier's legal and financial identity. Furthermore, the form asks for both the business and postal addresses, ensuring clear communication channels. The final sections of the form are designated for banking information, including account name, number, and type, which are crucial for processing payments accurately and efficiently. This registration process is safeguarded by a section that must be completed by a bank official, guaranteeing the legitimacy of the provided banking details. Suppliers are instructed to submit original documents to specified addresses, highlighting the form's role in formalizing the supplier's relationship with the department and ensuring a smooth transaction process for both parties.
| Question | Answer |
|---|---|
| Form Name | Logis Supplier Registration Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | logis, logis number state, how to get logis number, logis supplier registration form state |
LOGIS Supplier Registration Form
SUPPLIER DETAILS |
CREDIT ORDER INSTRUCTION |
COMPANY'S FULL TRADING NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
1. I/We hereby request and authorise you to pay any amounts which accrue to me/us to the |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
credit of my/our account with the mentioned bank. |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2. I/We understand that the credit transfer hereby authorised will be processed by Electronic |
||||||||||||||
|
|
|
|
|
|
|
(please print clearly) |
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Fund Transfer (EFT) and I/We also understand that no additional advice of payment will be |
||||||||||||||
|
|
|
Year |
|
|
|
Number |
Type |
|||||||||||||||||||||
ENTERPRISE REGISTRATION NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
provided other than the details of each payment as provided by my/our bank. |
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
3. This authority may be cancelled by me/us by giving thirty day's notice by |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
(Please attach a copy |
|
of the Registration Certificate) |
|
|
post or by hand delivered instruction. |
|
|
|
|
|
|
|
|
|
|
||||||||||
ID Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4. I/We will not hold the Eastern Cape Provincial Administration liable for any payment not made |
||||||||||||||
(If Sole Proprietor) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
into my/our bank account if the bank account details are incorrect or were not supplied to the |
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
(Please attach a copyofthe |
IDDocument) |
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
Department within a reasonable time prior to the expected date of payment, subject to |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
VAT NUMBER |
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
appropriate contracting or order procedures being followed. |
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5. The information provided for this registration as it applies to the supply of all goods and |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
services, and the related payment will be subject to the General Conditions of Contract or as |
||||||||||||||
BUSINESS ADDRESS |
Line 1: |
|
|
|
|
|
|
|
|
|
|
|
|
|
otherwise agreed with the relevant department. |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Line 2: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Telephone no |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
and area code: ( |
|
) |
|
|
|
|
|
|
|
|
|
|
|
Initials and Surname |
Authorised Signature |
|
|
Date |
|||||||||||
|
Fax no and area |
|
|
|
|
|
|
|
|
|
|
|
|
DETAILS OF MY/OUR BANK ACCOUNT |
|
|
|
|
|
||||||||||
code:( |
|
) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Bank |
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
||||
POSTAL ADDRESS |
Line 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
of |
|
|
|
|
|
|
|
|
|
|
||||
|
Line 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Branch Code |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
Postal Code |
|
|
|
|
|
Account Name |
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Account |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PAYMENT ADDRESS |
Line 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Number |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If Cheque |
a blank, canceled cheque |
|
|
|
|||||
|
Line 2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Account, attach |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Account Type: |
|
|
|
|
3 = Trans- |
4 = |
|
5 = |
6 = |
|
||||
|
City: |
|
|
|
|
|
|
Postal Code |
|
|
|
|
|
1 = Cheque Acc |
2 = Savings Acc |
mission Acc |
Bond Acc |
|
(Not in use) |
Acc |
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SARS personal identification number (PIN): ___________________ |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
Please complete this form and forward only original documents to: |
|
|
|
FOR INTERNAL USE ONLY |
|
|
|
|
|
|
FOR COMPLETION BY BANK OFFICIAL: |
|
|
|
|
|
|||||||||||||
Post to: |
|
|
By Hand: |
|
|
|
LOGIK Request Number: |
|
|
|
|
|
|
|
Bank account details are hereby certified as being correct: |
|
|
|
|||||||||||
SCMO: Logis Registrations |
SCMO: Logis Registrations |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
Provincial Planning and Treasury |
Provincial Planning and Treasury |
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
||||||
Private Bag X0029 |
|
Shop 5, Tyamzashe Building |
|
|
|
LOGIS Supplier Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Bhisho |
|
Phalo Avenue |
|
|
|
|
|
|
|
|
BANK STAMP WITH DATE |
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
5606 |
|
Bhisho |
|
|
|
|
|
|
|
|
|
|
|
|
|
ID Number: |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
CESD Number: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Signature: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|