
With the help of the online tool for PDF editing by FormsPal, you may fill out or change Form OCDD-PF-20-005 here and now. To retain our tool on the forefront of efficiency, we work to implement user-driven capabilities and enhancements on a regular basis. We're always thankful for any suggestions - play a vital part in reshaping PDF editing. It just takes several basic steps:
Step 1: Click the orange "Get Form" button above. It is going to open our editor so you could start filling in your form.
Step 2: Using this state-of-the-art PDF file editor, it's possible to do more than merely fill out blank form fields. Express yourself and make your docs look perfect with customized text added, or adjust the original content to excellence - all supported by the capability to insert any images and sign the PDF off.
This PDF doc needs specific details; to ensure accuracy and reliability, you need to consider the guidelines directly below:
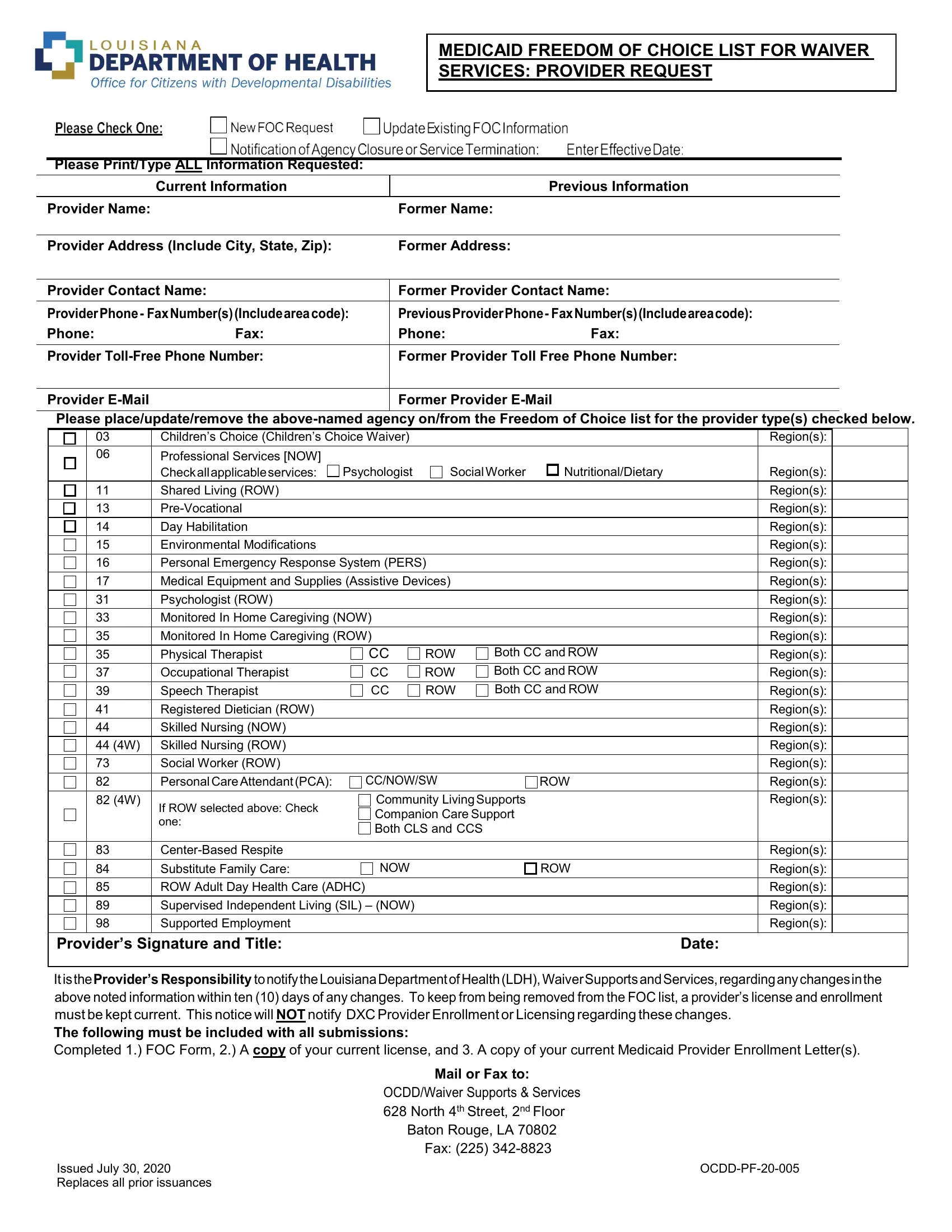
1. It is crucial to complete the Form OCDD-PF-20-005 accurately, so be mindful when filling out the segments including these particular blank fields:
2. Just after filling out the previous section, go on to the next stage and complete the essential details in these blank fields - PreVocational, Day Habilitation, Environmental Modifications, Personal Emergency Response System, Medical Equipment and Supplies, Psychologist ROW, Monitored In Home Caregiving NOW, Monitored In Home Caregiving ROW, Physical Therapist, Occupational Therapist, Speech Therapist, Registered Dietician ROW, Skilled Nursing NOW, CC CC, and ROW.
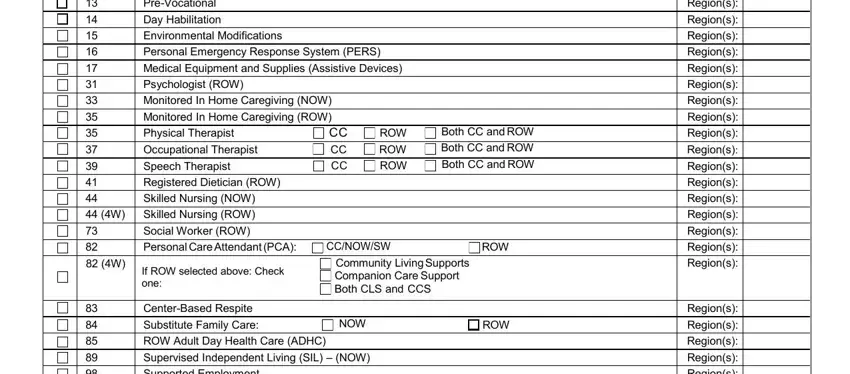
3. Through this part, look at Supported Employment, Regions, Providers Signature and Title, Date, It is the Providers Responsibility, Mail or Fax to, OCDDWaiver Supports Services, Baton Rouge LA Fax, Issued July Replaces all prior, and OCDDPF. Each one of these should be filled in with highest attention to detail.
Be really attentive while filling out Mail or Fax to and Providers Signature and Title, as this is where most users make a few mistakes.
Step 3: Prior to moving on, check that all blanks were filled in properly. Once you establish that it's good, press “Done." Join us now and instantly obtain Form OCDD-PF-20-005, all set for download. Every single modification made is handily saved , helping you to edit the form later on if necessary. We do not share or sell any information you enter while dealing with forms at FormsPal.