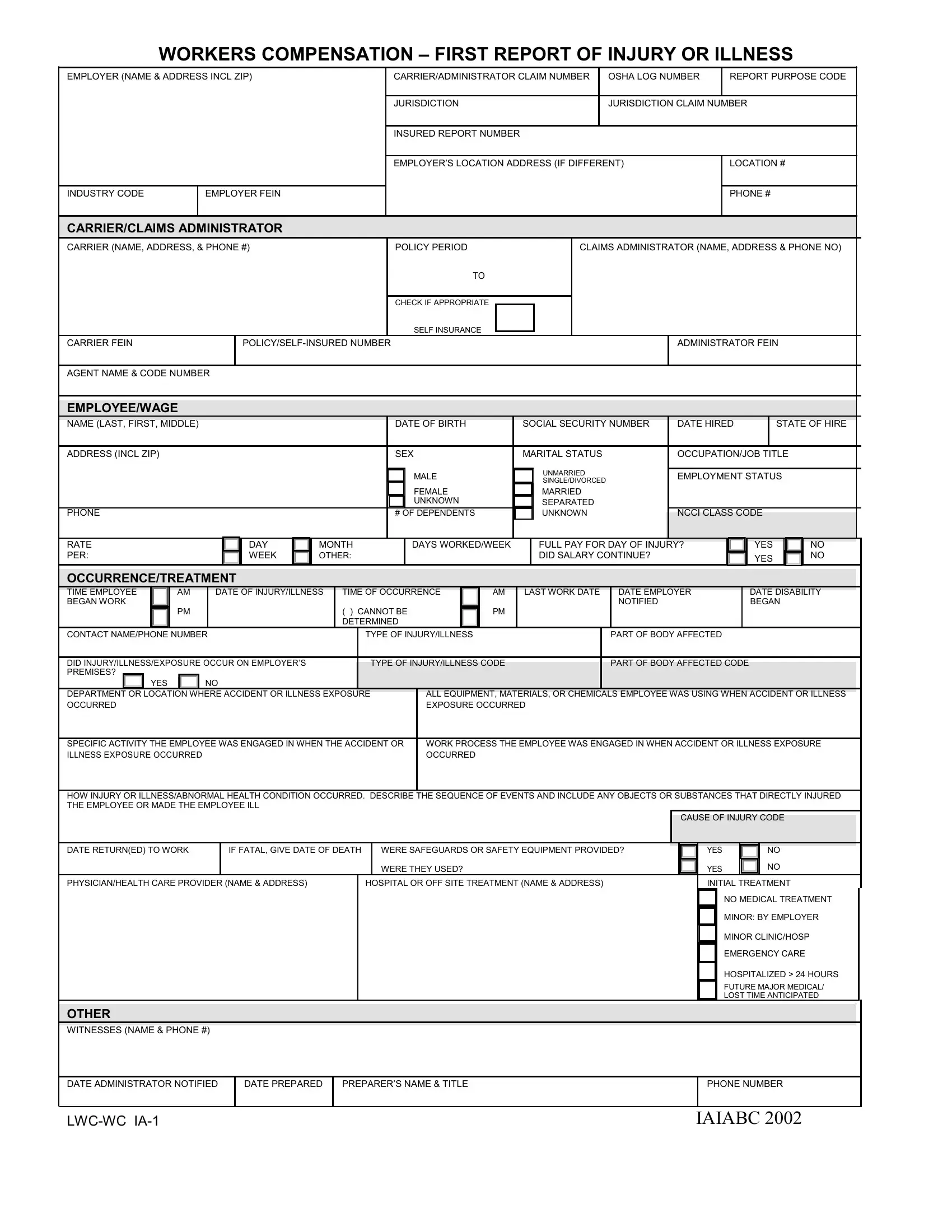
At the crux of workplace safety and insurance reporting in the context of workers' compensation lies the critical document, the LWC WC IA-1 form or the Workers Compensation – First Report of Injury or Illness. This comprehensive form serves as a preliminary notification detailing an employee's job-related injury or illness, marking the inception of a potentially complex process involving multiple stakeholders including employers, insurance carriers, and healthcare providers. It compels the employer to furnish pertinent details, such as the employer's and employee's information, the latter including name, date of birth, social security number, and specifics about the employment and the incident like date hired, occupation, and a detailed account of the injury or illness event. The necessity for this document extends beyond mere procedural adherence; it encapsulates essential data required by insurance entities to initiate a claim, ensuring that employees receive appropriate medical attention and compensation for lost wages. With sections dedicated to the cause of injury, nature of illness, and initial treatment, the form acts as a cornerstone for the administration of workers' compensation benefits, making accurate and timely completion paramount. Moreover, it underscores the employer's role in maintaining a safe work environment, highlighting whether safety measures were provided and adhered to at the time of the incident. Through this form, a framework is established not only for reporting but also for analyzing workplace safety, potentially guiding future efforts to mitigate risks and foster a healthier, more secure work setting.
| Question | Answer |
|---|---|
| Form Name | Lwc Wc Ia 1 Form |
| Form Length | 3 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 45 sec |
| Other names | louisiana workers injury, lwc workers compensation, first report injury, first report of injury |
WORKERS COMPENSATION – FIRST REPORT OF INJURY OR ILLNESS
EMPLOYER (NAME & ADDRESS INCL ZIP)
INDUSTRY CODE |
EMPLOYER FEIN |
|
|
CARRIER/ADMINISTRATOR CLAIM NUMBER |
OSHA LOG NUMBER |
|
REPORT PURPOSE CODE |
|
|
|
|
JURISDICTION |
JURISDICTION CLAIM NUMBER |
||
INSURED REPORT NUMBER |
|
|
|
|
|
|
|
EMPLOYER’S LOCATION ADDRESS (IF DIFFERENT) |
|
LOCATION # |
|
|
|||
|
|
|
|
|
|
|
PHONE # |
|
|
|
|
CARRIER/CLAIMS ADMINISTRATOR
CARRIER (NAME, ADDRESS, & PHONE #) |
POLICY PERIOD |
TO
CHECK IF APPROPRIATE
SELF INSURANCE
CARRIER FEIN |
|
|
|
AGENT NAME & CODE NUMBER
CLAIMS ADMINISTRATOR (NAME, ADDRESS & PHONE NO)
ADMINISTRATOR FEIN
EMPLOYEE/WAGE
NAME (LAST, FIRST, MIDDLE) |
DATE OF BIRTH |
SOCIAL SECURITY NUMBER |
DATE HIRED |
STATE OF HIRE |
|
|
|
|
|
ADDRESS (INCL ZIP) |
SEX |
MARITAL STATUS |
OCCUPATION/JOB TITLE |
|
|
|
M |
MALE |
U |
UNMARRIED |
EMPLOYMENT STATUS |
|
|
|
|
SINGLE/DIVORCED |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
F |
FEMALE |
M |
MARRIED |
|
|
|
|
|
U |
UNKNOWN |
S |
SEPARATED |
|
|
|
PHONE |
|
# OF DEPENDENTS |
K |
UNKNOWN |
NCCI CLASS CODE |
|
||
RATE |
DAY |
MONTH |
DAYS WORKED/WEEK |
|
FULL PAY FOR DAY OF INJURY? |
YES |
NO |
|
PER: |
WEEK |
OTHER: |
|
|
DID SALARY CONTINUE? |
|
YES |
NO |
|
|
|
|
|
|
|
|
|
OCCURRENCE/TREATMENT
|
|
|
|
|
|
|
|
|
|
|
|
TIME EMPLOYEE |
AM |
DATE OF INJURY/ILLNESS |
TIME OF OCCURRENCE |
AM |
LAST WORK DATE DATE EMPLOYER |
DATE DISABILITY |
|||||
BEGAN WORK |
|
|
|
|
|
|
|
NOTIFIED |
BEGAN |
||
PM |
( ) CANNOT BE |
PM |
|
DETERMINED |
|
CONTACT NAME/PHONE NUMBER |
TYPE OF INJURY/ILLNESS |
|
PART OF BODY AFFECTED |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
DID INJURY/ILLNESS/EXPOSURE OCCUR ON EMPLOYER’S |
|
|
|
|
|
|
|||||
|
TYPE OF INJURY/ILLNESS CODE |
PART OF BODY AFFECTED CODE |
|
||||||||
PREMISES? |
|
|
|
|
|
|
|
|
|
|
|
|
|
YES |
|
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE |
|
ALL EQUIPMENT, MATERIALS, OR CHEMICALS EMPLOYEE WAS USING WHEN ACCIDENT OR ILLNESS |
|
||||||||
OCCURRED |
|
|
|
EXPOSURE OCCURRED |
|
|
|
||||
|
|
|
|
|
|
|
|||||
SPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR |
WORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS EXPOSURE |
|
|||||||||
ILLNESS EXPOSURE OCCURRED |
|
|
|
OCCURRED |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
HOW INJURY OR ILLNESS/ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILL
CAUSE OF INJURY CODE
DATE RETURN(ED) TO WORK |
IF FATAL, GIVE DATE OF DEATH |
|
|
WERE SAFEGUARDS OR SAFETY EQUIPMENT PROVIDED? |
|
|
|
|
|
|
WERE THEY USED? |
|
|
|
|
||
PHYSICIAN/HEALTH CARE PROVIDER (NAME & ADDRESS) |
|
HOSPITAL OR OFF SITE TREATMENT (NAME & ADDRESS) |
|||
|
|
|
|
|
|
OTHER
WITNESSES (NAME & PHONE #)
YES NO
YES |
|
NO |
INITIAL TREATMENT |
||
0 |
NO MEDICAL TREATMENT |
|
1 |
MINOR: BY EMPLOYER |
|
2 |
MINOR CLINIC/HOSP |
|
3 |
EMERGENCY CARE |
|
|
||
4 |
HOSPITALIZED > 24 HOURS |
|
5 |
FUTURE MAJOR MEDICAL/ |
|
LOST TIME ANTICIPATED |
||
|
||
DATE ADMINISTRATOR NOTIFIED |
DATE PREPARED |
PREPARER’S NAME & TITLE |
|
|
|
PHONE NUMBER
IAIABC 2002
EMPLOYER’S INSTRUCTIONS
DO NOT ENTER DATA IN SHADED FIELDS
DATES:
Enter all dates in MM/DD/YY format.
INDUSTRY CODE:
This is the code which represents the nature of the employer’s business, which is contained in the Standard Industrial Classification Manual or the North American Industry Classification System, published by the Federal Office of Management and Budget.
CARRIER:
The licensed business entity issuing a contract of insurance and assuming financial responsibility on behalf of the employer of the claimant.
CLAIMS ADMINISTRATOR:
Enter the name of the carrier, third party administrator, state fund, or
AGENT NAME & CODE NUMBER:
Enter the name of your insurance agent and his/her code number if known. This information can be found on your insurance policy.
OCCUPATION/JOB TITLE:
This is the primary occupation of the claimant at the time of the accident or exposure.
EMPLOYMENT STATUS: |
|
|
|
Indicate the employee’s work status. The valid choices are: |
|
||
On Strike |
Unknown |
Volunteer |
|
Disabled |
Apprenticeship |
Seasonal |
|
Not Employed |
Retired |
Apprenticeship |
Piece Worker |
DATE DISABILITY BEGAN:
The first day on which the claimant originally lost time from work due to the occupation injury or disease or as otherwise designated by statute.
CONTACT NAME/PHONE NUMBER:
Enter the name of the individual at the employer’s premises to be contacted for additional information.
TYPE OF INJURY/ILLNESS:
Briefly describe the nature of the injury or illness, (eg. Lacerations to the forearm).
PART OF BODY AFFECTED:
Indicate the part of body affected by the injury/illness, (eg. Right forearm, lower back).
DEPARTMENT OR LOCATION WHERE ACCIDENT OR ILLNESS EXPOSURE OCCURRED: (eg. Maintenance Department or Client’s office at 452 Monroe St., Washington, DC 26210)
If the accident or illness exposure did not occur on the employer’s premises, enter address or location. Be specific.
IAIABC 2002 |
EMPLOYER’S INSTRUCTIONS – cont’d
ALL EQUIPMENT, MATERIAL OR CHEMICALS EMPLOYEE WAS USING WHEN ACCIDENT OR ILLNESS EXPOSURE OCCURRED:
(eg. Acetylene cutting torch, metal plate)
List all of the equipment, materials, and/or chemicals the employee was using, applying, handling or operating when the injury or illness occurred. Be specific, for example: decorator’s scaffolding, electric sander, paintbrush, and paint.
Enter “NA” for not applicable if no equipment, materials, or chemicals were being used. NOTE: The items listed do not have to be directly involved in the employee’s injury or illness.
SPECIFIC ACTIVITY THE EMPLOYEE WAS ENGAGED IN WHEN THE ACCIDENT OR ILLNESS EXPOSURE OCCURRED:
(eg. Cutting metal plate for flooring)
Describe the specific activity the employee was engaged in when the accident or illness exposure occurred, such as sanding ceiling woodwork in preparation for painting.
WORK PROCESS THE EMPLOYEE WAS ENGAGED IN WHEN ACCIDENT OR ILLNESS EXPOSURE OCCURRED: Describe the work process the employee was engaged in when the accident or illness exposure occurred, such as building maintenance. Enter “NA” for not applicable if employee was not engaged in a work process (eg. walking along a hallway).
HOW INJURY OR ILLNESS/ABNORMAL HEALTH CONDITION OCCURRED. DESCRIBE THE SEQUENCE OF EVENTS AND INCLUDE ANY OBJECTS OR SUBSTANCES THAT DIRECTLY INJURED THE EMPLOYEE OR MADE THE EMPLOYEE ILL:
(Worker stepped back to inspect work and slipped on some scrap metal. As worker fell, worker brushed against the hot metal.)
Describe how the injury or illness/abnormal health condition occurred. Include the sequence of events and name any objects or substance that directly injured the employee or made the employee ill. For example: Worker stepped to the edge of the scaffolding to inspect work, lost balance and fell six feet to the floor. The worker’s right wrist was broken in the fall.
DATE RETURN(ED) TO WORK:
Enter the date following to most recent disability period on which the employee returned to work.