Maintaining comprehensive records for the health and welfare of horses is paramount for owners, riders, and caretakers. The Maintenance Book form, provided by The United States Pony Club, Inc., offers a meticulous approach to this crucial aspect. From basic identifiers like the horse's name, breed, and physical characteristics to more detailed accounts of medical conditions, vaccination schedules, and deworming records, this form encompasses all facets of equine care. It extends beyond health, covering the horse's living conditions, including the facility's name and contact information for the veterinarian and farrier, ensuring all caretaking needs are well-documented. Moreover, the form highlights the importance of emergency preparedness with sections for insurance details and emergency contact numbers. The inclusion of a place for visual identification, both through a drawn diagram and a photograph, further underscores the form's comprehensiveness. By organizing horse health and maintenance data in one place, the Maintenance Book form serves as an essential tool for ensuring the well-being and proper care of horses, reflecting the commitment of The United States Pony Club to the equine community.
| Question | Answer |
|---|---|
| Form Name | Maitenance Book Form |
| Form Length | 15 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 3 min 45 sec |
| Other names | pony club record book, uspc health and maintenance record book, pony club record book blank, uspc record book |
Health & Maintenance Records for
Horse:
The United States Pony Club, Inc.
Name:
Pony Club:
Region:
Start Date: |
|
End Date: |
|
|
|
|
|

General Information
Rider: |
|
|
|
|
|
|
|
|
D.O.B: |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
Phone #: ( |
) |
|
||||
|
|
|
|
|
|
|
|
|
|
||||||||
Owner: |
|
|
|
|
|
|
|
|
|
|
|||||||
Address: |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Phone #’s: ( |
) |
( |
|
|
) |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
Horse’s Location |
|
|
|
|
|
|
|
||||||||||
Name of Facility: |
|
|
|
|
|
|
|
||||||||||
Address: |
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Phone #: ( |
) |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
Veterinarian: |
|
|
Phone #: ( |
) |
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||
Farrier: |
|
|
|
Phone #: ( |
) |
|
|||||||||||
|
|
|
|
|
|
|
|
||||||||||
Other: |
|
|
|
|
Phone #: ( |
) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Insurance (Horse)
Carrier Name:
Policy #:
Phone #: ( |
) |
||
|
|
|
|
Emergency #: ( |
) |
||
|
|
|
|
1
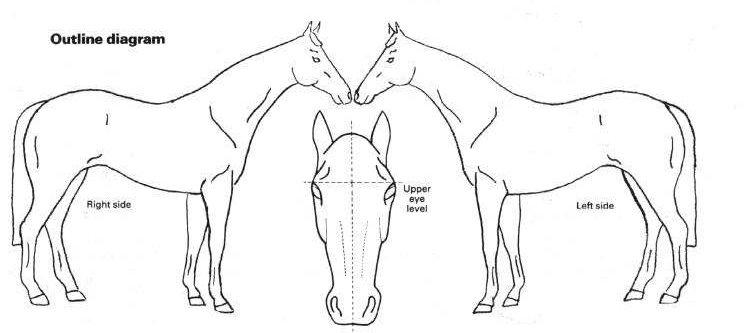
Draw in markings and brands on the diagram above.
Please place a photograph in the space below for identification purposes.
(This picture should be standing and in profile.)
2
Horse Information
Horse’s Name: |
|
|
|
|
|
Date Foaled.: |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Height: |
|
Color: |
Breed: |
|
Sex: _____ |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
Weight: |
Markings: |
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Tatoo/Brands:
Vital Signs At Rest:
Temperature: |
|
Pulse: |
Respiration:_____ |
|
|
|
|
|
|
Vices:
Special Medical Conditions:
Inoculation Schedule
Please list what vaccinations your horse gets and on what schedule:____________
__________________________________________________________________
__________________________________________________________________
__________________________________________________________________
Breed Registry:
Registration #:
Sire:
Dam:
3
Date
|
|
Routine |
||
Immunizations |
|
|
|
|
Vaccine |
|
Due Again |
|
Cost |
|
|
|||
|
|
on: |
|
|
Total $:
Date
Type of Wormer
Due Again
on:
Cost
4 |
Total $: |
Procedures
Shoeing
Date
Type of Shoes
Next
Appointment
Cost
Total $:
Dentistry
Date
Procedure/Comments
on:(date)
Cost
Total $:
5
Feed Schedule
AM: |
Roughage: |
|
|||
|
Concentrate: |
||||
NOON: |
Roughage: |
|
|
||
|
Concentrate: |
||||
PM: |
Roughage: |
|
|
||
|
Concentrates: |
|
|||
Supplements AM:____
Supplements PM: ___________________________________________
Salt Source:
Feed Changes
Date
Change From:
Change To:
6
Conditioning Schedule
(You may need to make additional copies of this page)
Conditioning Schedule for an average week:
Activity
Specifications
Average Minutes
Times/ Week
Temperature: @rest: |
Pulse: @rest: |
Respiration: @rest: |
||||||
|
|
|
|
|
|
|
|
|
@work: |
|
@work: |
|
@work: |
|
|||
Conditioning Changes
Date
Change From:
Change To:
TPR
Changes
7
Activities
( lessons, clinics, competitions, etc.)
Date
Activity
Comments
Cost
8
Activities
Date
Activity
Comments
Cost
Total $:
9
Extra Veterinary Visits
Includes: lameness, sickness,
Date
Description
Diagnosis & Treatment
Cost
Total $:
10
Feed and Board Expenses
Date
Item
Cost
Total $:
11
Other Expenses
Includes: travel expenses, tack, equipment, etc.
Date
Item
Cost
Total $:
12
Date
Income
(all sources)
Description
Amount
Total $:< |
> |
13
|
Expense Summary |
|
Totals from: |
|
|
Pg. 4: |
Immunizations: |
$ |
|
$ |
|
Pg. 5: |
Shoeing: |
$ |
|
Dentistry: |
$ |
Pg. 9: |
Activities |
$ |
Pg. 10: |
Extra Veterinary |
$ |
Pg. 11: |
Feed and Board |
$ |
Pg. 12: |
Other |
$ |
|
Total Expenses: $ |
|
|
|
|
- |
|
|
|
Pg. 13: |
Total Income: $< |
> |
|
|
|
|
|
|
|
Net Expenses: $
14