
 general internal medicine
general internal medicine 
 pediatric medicine
pediatric medicineThis PDF editor makes it simple to complete forms. You won't need to perform much to change aca 1202 physician certification and attestation fillable form forms. Only consider all of these actions.
Step 1: Press the button "Get form here" to open it.
Step 2: You're now on the form editing page. You can edit, add information, highlight selected words or phrases, insert crosses or checks, and insert images.
The PDF form you plan to fill in will contain the following sections:
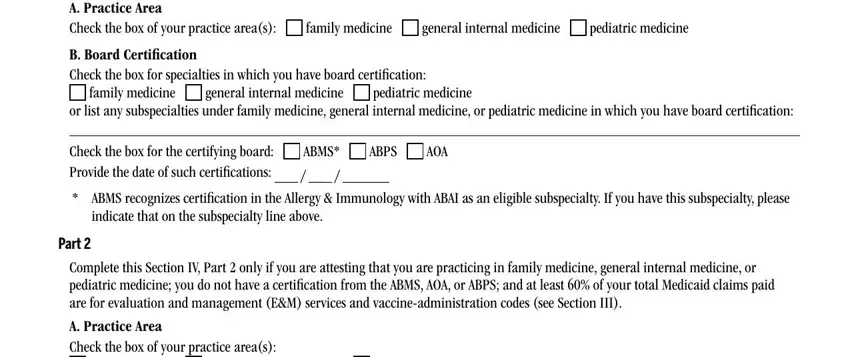
You should fill in the Complete this Section IV Part if, general internal medicine, pediatric medicine, family medicine, B Board Certification Check the box, family medicine, general internal medicine, pediatric medicine, or list any subspecialties under, Check the box for the certifying, ABMS, ABPS, AOA, indicate that on the subspecialty, and Part space with the required particulars.
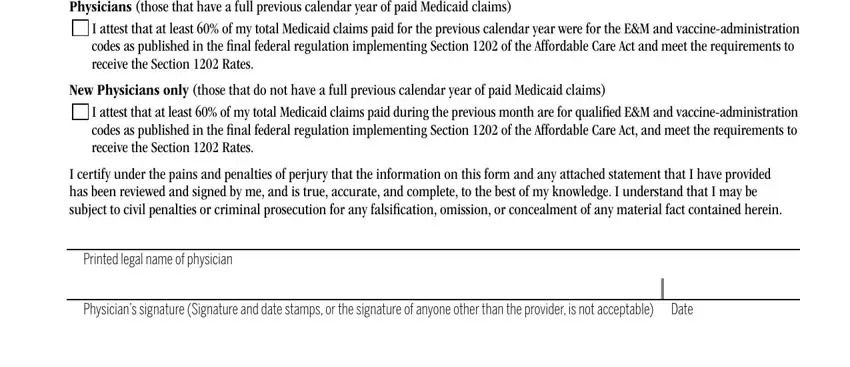
Mention the important data in B Paid Claims Physicians those, I attest that at least of my, New Physicians only those that do, I attest that at least of my, I certify under the pains and, Printed legal name of physician, and Physicians signature Signature and section.
Step 3: The moment you hit the Done button, your completed document is simply exportable to every of your devices. Or alternatively, you may send it through email.
Step 4: To protect yourself from any problems in the foreseeable future, you should have at least a couple of copies of the file.
