
With the help of the online tool for PDF editing by FormsPal, you can fill out or modify virginia school entrance health form right here and now. FormsPal is dedicated to providing you the ideal experience with our tool by consistently releasing new functions and upgrades. With these updates, working with our editor becomes better than ever before! To get the process started, go through these basic steps:
Step 1: Firstly, open the pdf tool by clicking the "Get Form Button" at the top of this page.
Step 2: When you start the file editor, you'll see the document ready to be completed. Besides filling in various blanks, you can also do other sorts of things with the PDF, particularly adding any textual content, editing the initial text, adding illustrations or photos, signing the PDF, and more.
Pay close attention when filling in this document. Make certain every single field is filled out correctly.
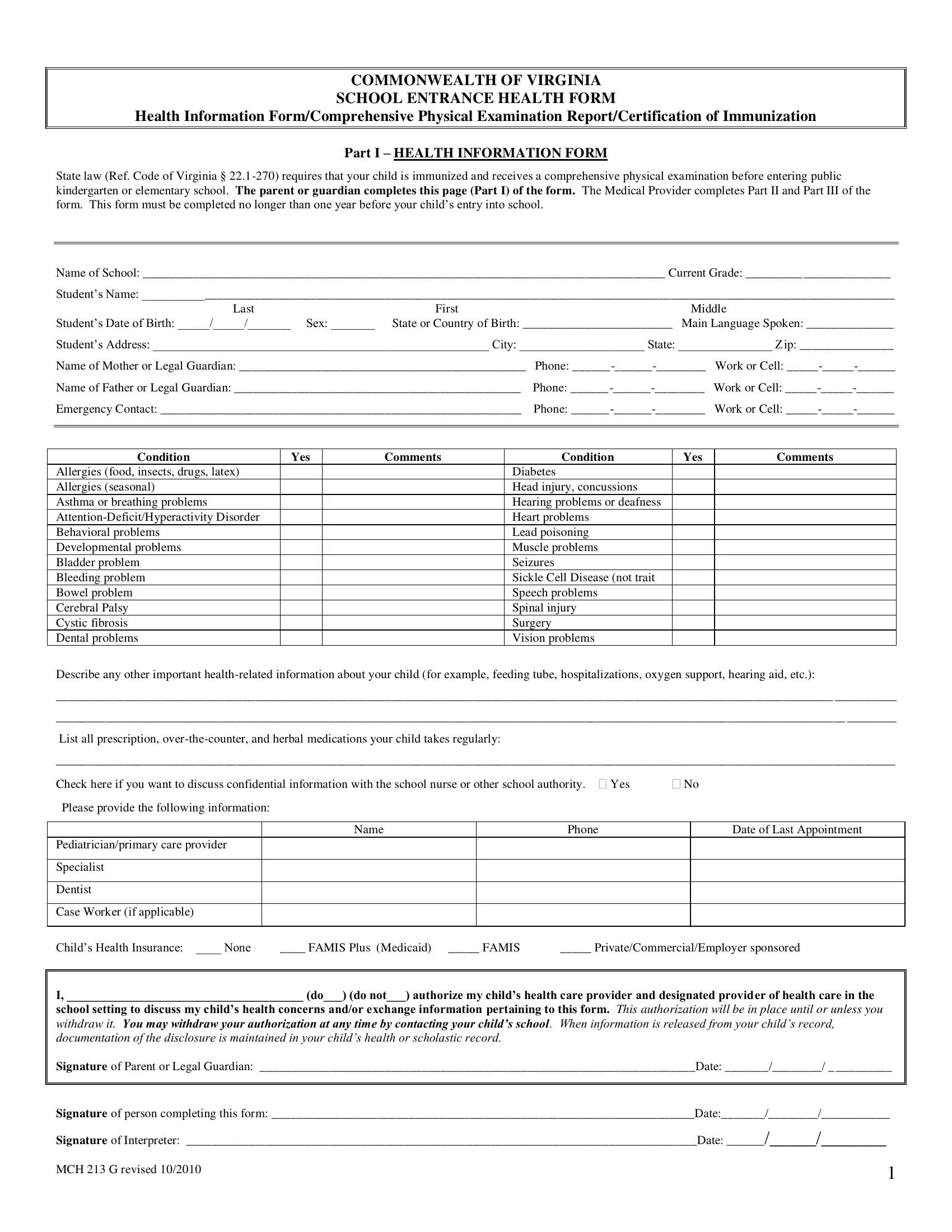
1. To get started, once filling in the virginia school entrance health form, start with the section that contains the next fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Describe any other important, List all prescription, Check here if you want to discuss, Yes, Please provide the following, Name, Phone, Date of Last Appointment, Pediatricianprimary care provider, Specialist, Dentist, Case Worker if applicable, Childs Health Insurance None, FAMIS Plus Medicaid, and FAMIS with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. Completing First, Middle, Last, IMMUNIZATION, RECORD COMPLETE DATES month day, A copy of the immunization record, Serological Confirmation of, and Serological Confirmation of is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
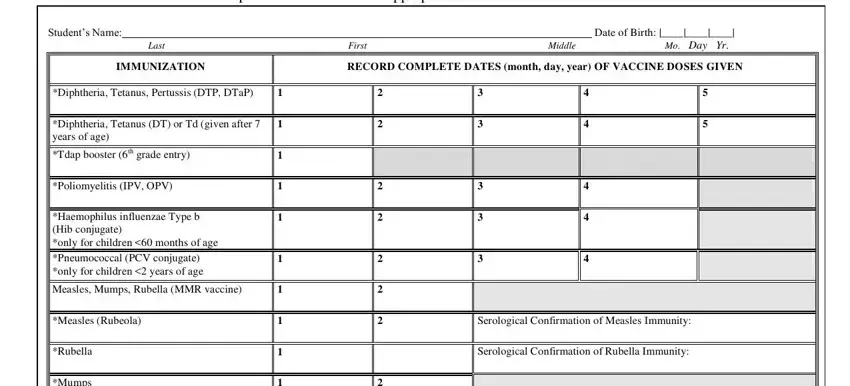
As for RECORD COMPLETE DATES month day and Serological Confirmation of, be certain you double-check them here. Those two are definitely the most significant fields in this PDF.
4. All set to proceed to this fourth form section! Here you have all these A copy of the immunization record, Date of Varicella Disease OR, Merck adult formulation used, and MCH G revised empty form fields to complete.
5. To wrap up your document, this particular part incorporates a few additional blanks. Filling in Students Name Date of Birth, Section II, Conditional Enrollment and, Complete the medical exemption or, MEDICAL EXEMPTION As specified in, and RELIGIOUS EXEMPTION The Code of will finalize everything and you can be done quickly!
Step 3: Immediately after proofreading your filled in blanks, hit "Done" and you're all set! Make a free trial plan at FormsPal and get instant access to virginia school entrance health form - downloadable, emailable, and editable in your personal account. FormsPal offers safe document tools devoid of personal information record-keeping or any sort of sharing. Feel at ease knowing that your information is in good hands here!