Our best computer programmers worked hard to design the PDF editor we're happy to deliver to you. The software enables you to quickly create med 9 form denver human services and saves your time. You need to simply try out this guideline.
Step 1: Select the button "Get Form Here" on the following website and next, click it.
Step 2: Right now, you may modify the med 9 form denver human services. The multifunctional toolbar makes it easy to insert, erase, modify, highlight, and also undertake other commands to the content and areas inside the form.
Enter the details requested by the application to complete the document.
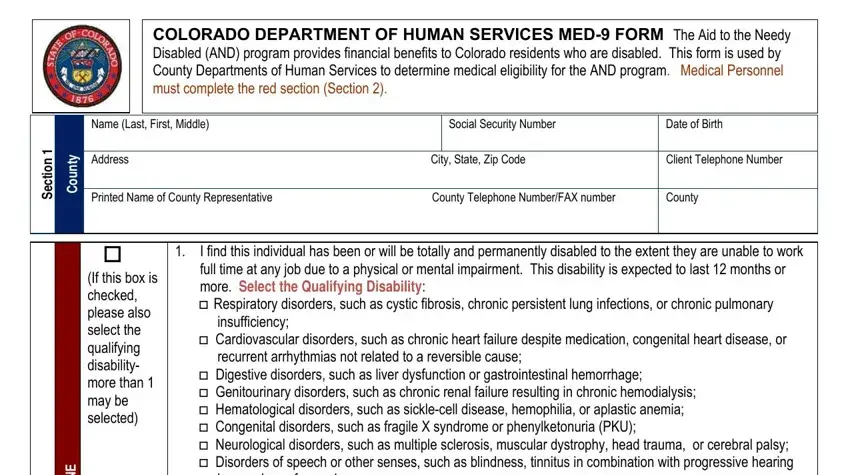
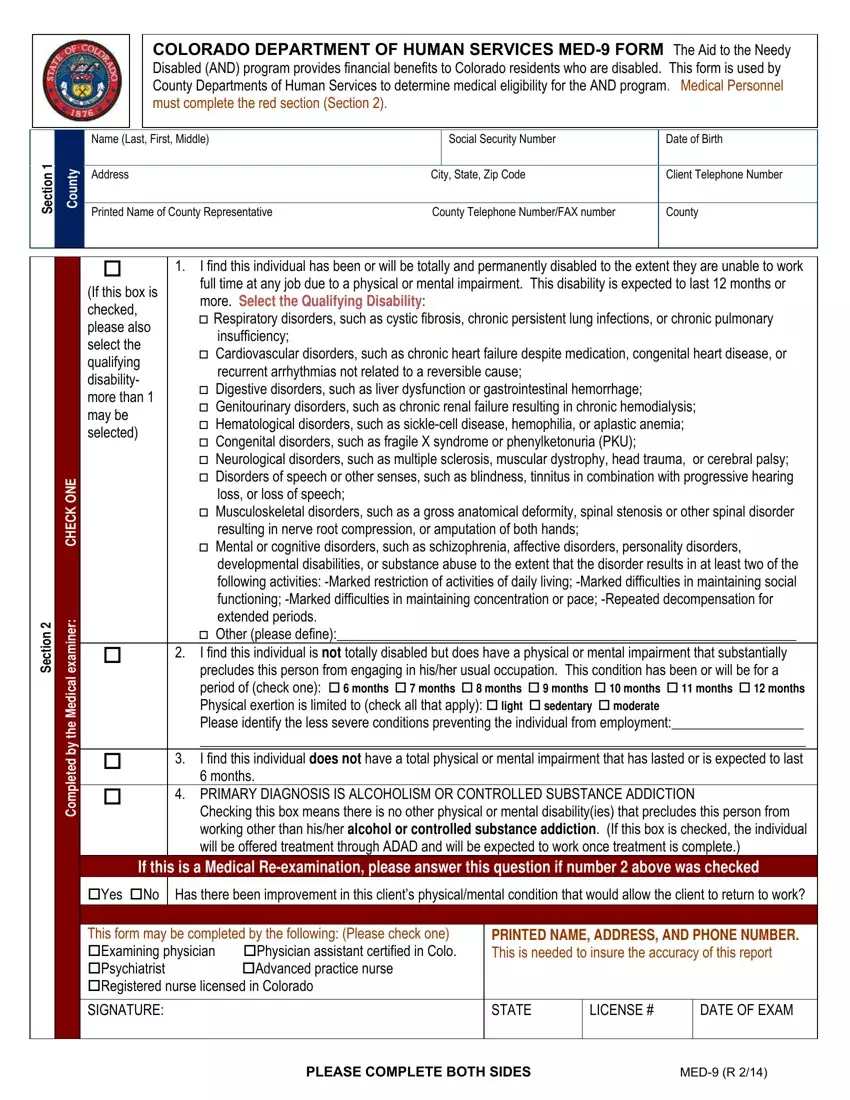
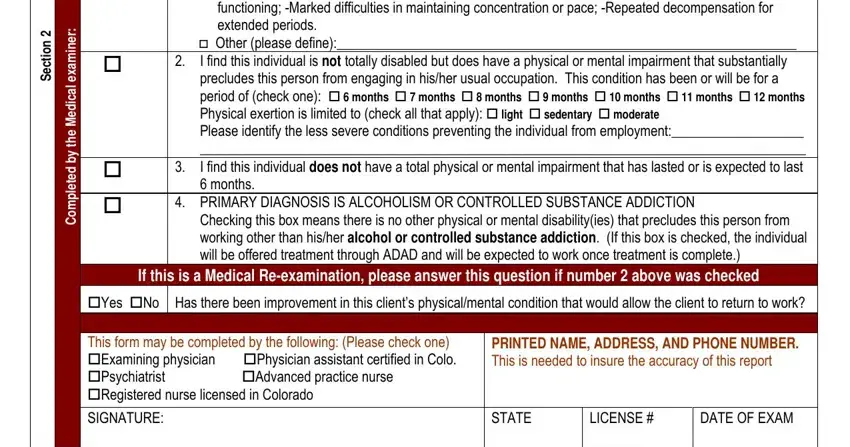
Type in the information in the n o i t c e S, r e n m a x e l a c i d e M e h t, developmental disabilities or, Other please define I find this, PRIMARY DIAGNOSIS IS ALCOHOLISM, Checking this box means there is, Yes No Has there been improvement, This form may be completed by the, PRINTED NAME ADDRESS AND PHONE, SIGNATURE, STATE, LICENSE, and DATE OF EXAM field.
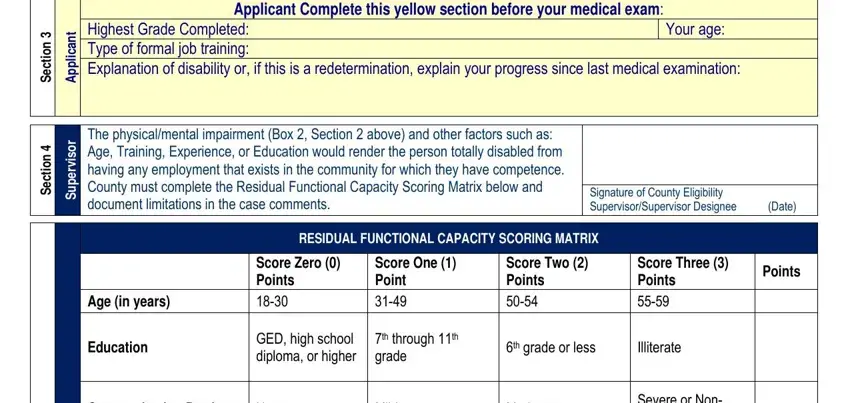
The program will request details to easily submit the segment Applicant Complete this yellow, Highest Grade Completed Type of, Your age, n o i t c e S, t n a c i l, p p A, The physicalmental impairment Box, n o i t c e S, r o s i v r e p u S, Age Training Experience or, Signature of County Eligibility, Age in years, Education, RESIDUAL FUNCTIONAL CAPACITY, and Score Zero Points.
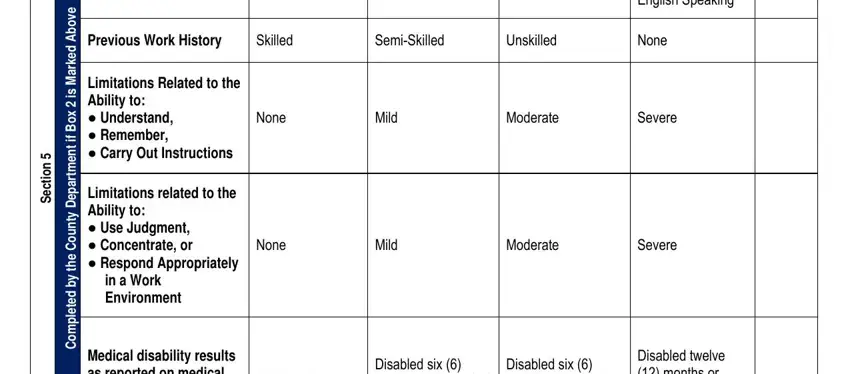
The field n o i t c e S, e v o b A d e k r a M s i x o B, f i, t n e m, t r a p e D y t n u o C e h t y b, Communication Barriers, None, Mild, Moderate, Severe or Non English Speaking, Previous Work History, Skilled, SemiSkilled, Unskilled, and None is for you to indicate all parties' rights and responsibilities.
Finalize by reviewing these areas and filling out the pertinent information: TOTAL RESIDUAL FUNCTIONAL CAPACITY, PLEASE COMPLETE BOTH SIDES, and MED R.

Step 3: After you've selected the Done button, your file will be accessible for transfer to any kind of device or email address you specify.
Step 4: Generate copies of your form - it will help you remain away from potential complications. And fear not - we are not meant to publish or see your information.
