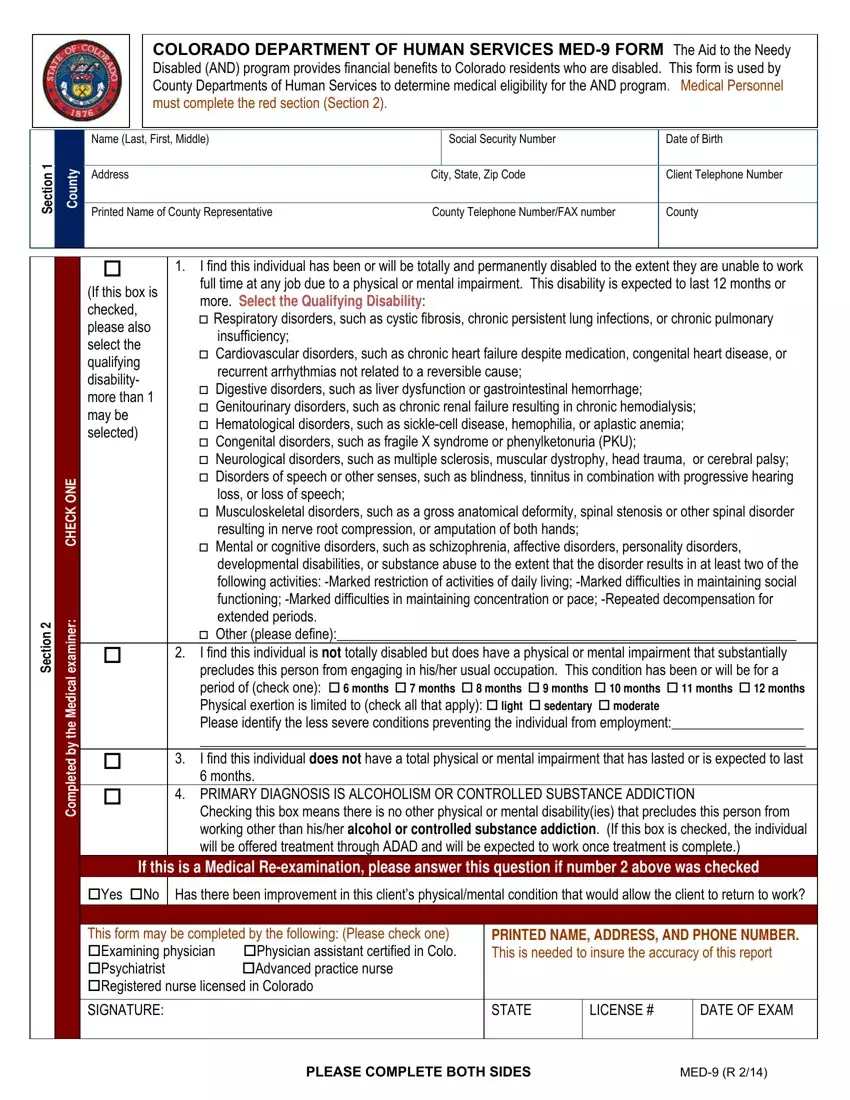
The MED-9 form, governed by the Colorado Department of Human Services, plays a pivotal role in the Aid to the Needy Disabled (AND) program, designed to provide financial support to residents facing disabilities that deter them from gainful employment. This comprehensive document bridges the critical assessment of medical eligibility for the AND program by county departments and healthcare professionals. With a detailed structure that guides medical personnel through a red section dedicated to their insights, the form solicits information regarding the claimant's disability, including a broad spectrum of qualifying conditions such as respiratory, cardiovascular, and neurological disorders, among others. It meticulously outlines the severity of the disability, whether total and permanent or substantial yet not fully preclusive of work, setting the stage for a clear communication relay between medical evaluators and county representatives. Further, the form navigates through the applicant's personal information, ensuring a holistic approach to understanding their condition. By encapsulating primary diagnoses, levels of physical exertion, and an evaluation of how a disability may impede work activities, the MED-9 form stands as a cornerstone in the decision-making process for the AND program, aiming to accurately channel benefits to those in dire need based on a structured medical and functional capacity assessment.
| Question | Answer |
|---|---|
| Form Name | Med 9 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | colorado med9 form, med 9 form colorado 2021, med 9 form denver human services, colorado department of human services med 9 |
