
You'll be able to work with PTAN easily by using our PDF editor online. FormsPal development team is always working to enhance the tool and ensure it is much faster for users with its multiple functions. Uncover an ceaselessly progressive experience today - check out and uncover new possibilities as you go! To begin your journey, take these simple steps:
Step 1: First, open the editor by clicking the "Get Form Button" in the top section of this page.
Step 2: This editor provides the ability to modify PDF files in a variety of ways. Change it with your own text, adjust what's already in the file, and include a signature - all manageable within minutes!
Concentrate while filling out this form. Make sure every single blank is filled in accurately.
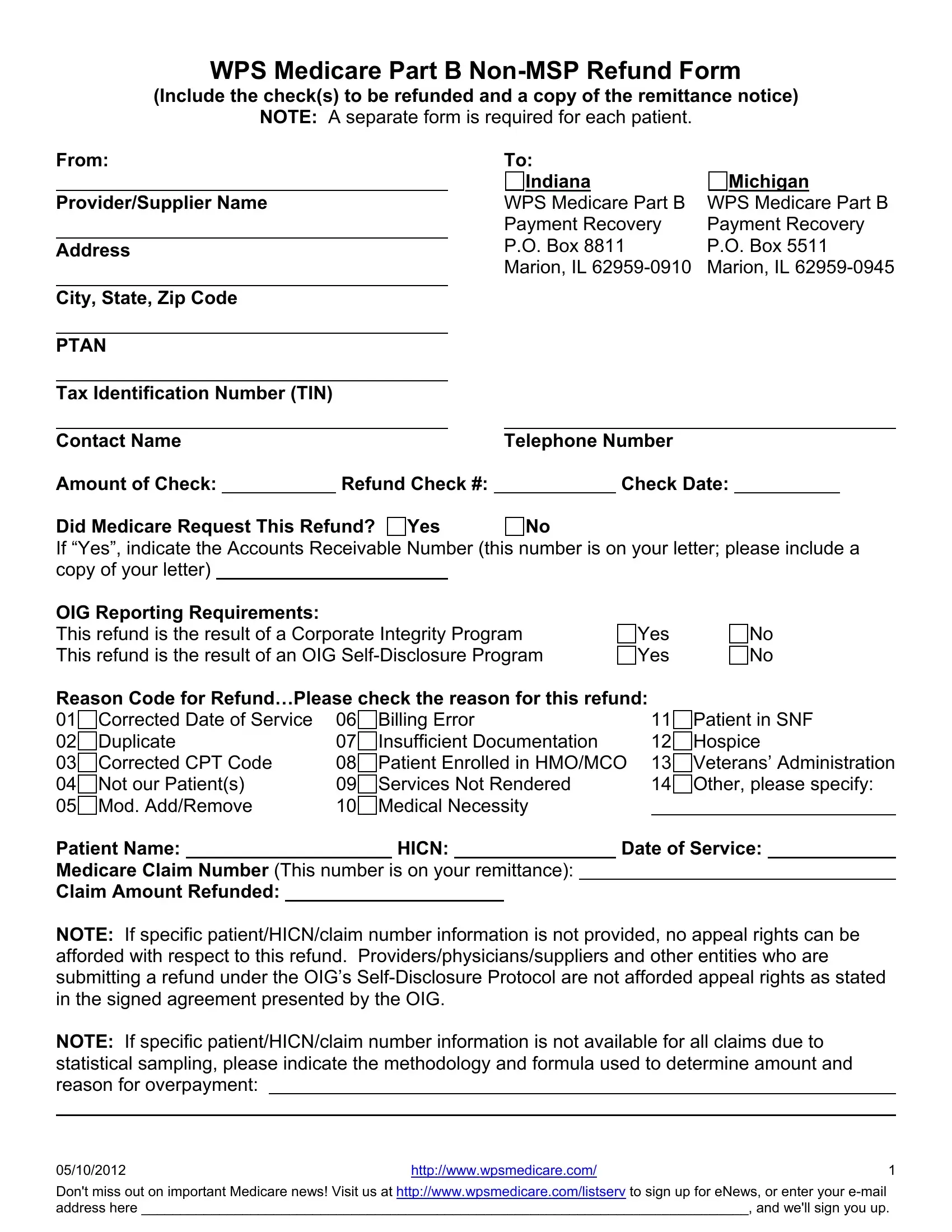
1. Begin completing your PTAN with a number of essential fields. Gather all the required information and ensure absolutely nothing is neglected!
2. Soon after this part is completed, go to enter the relevant information in all these: From ProviderSupplier Name Address, Patient in SNF Hospice Veterans, Insufficient Documentation, Date of Service, HICN, Yes Yes, and No No.
3. Completing Dont miss out on important, and httpwwwwpsmedicarecom is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!

People who work with this document frequently get some points incorrect while filling out httpwwwwpsmedicarecom in this area. You need to read again everything you type in right here.
Step 3: Before finalizing the document, make certain that blanks have been filled out as intended. The moment you verify that it is correct, press “Done." Right after getting a7-day free trial account here, you'll be able to download PTAN or send it through email at once. The PDF file will also be at your disposal from your personal account menu with your edits. FormsPal is invested in the confidentiality of our users; we make sure that all personal data entered into our tool remains protected.