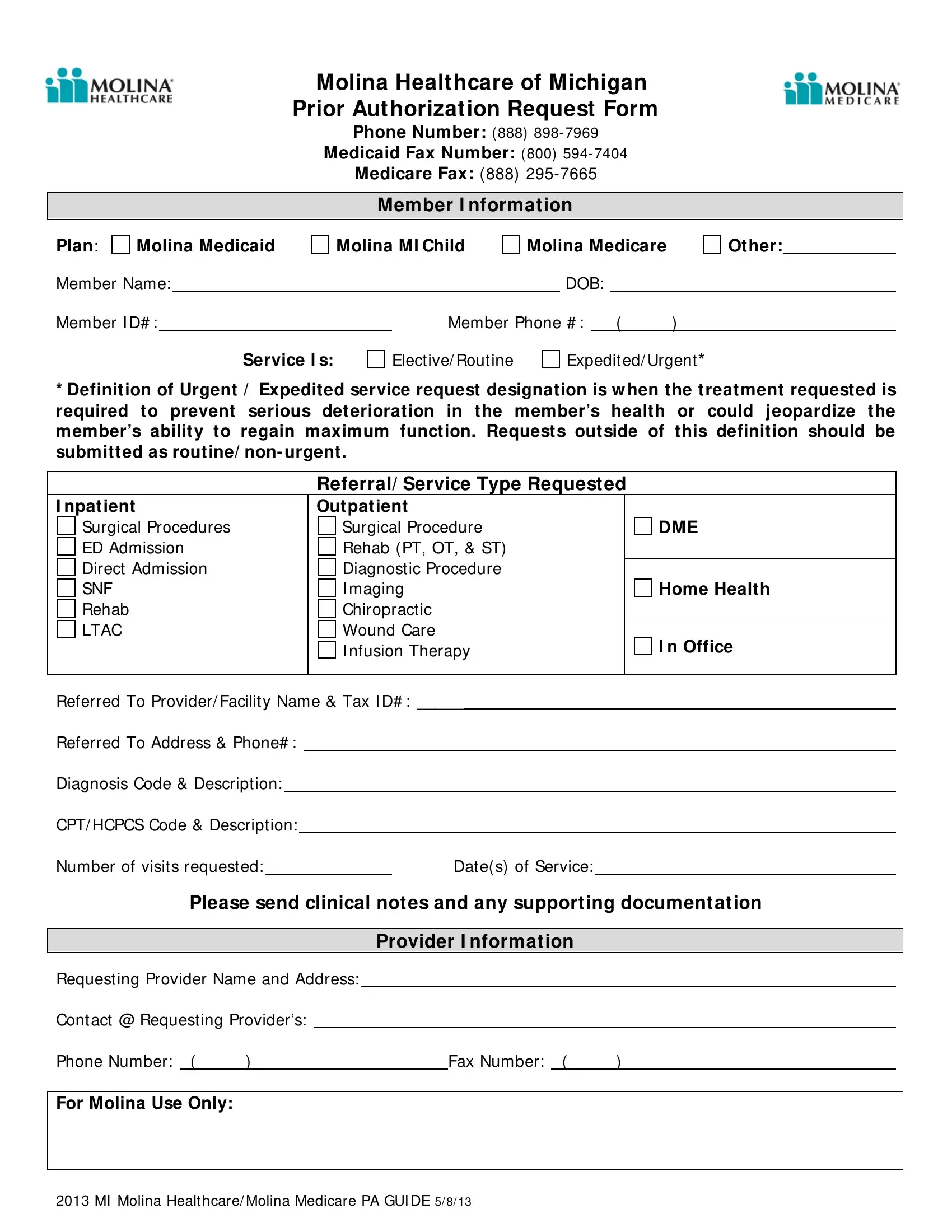
The Michigan Molina Prior Authorization Request Form serves as a critical conduit between healthcare providers and Molina Healthcare of Michigan, ensuring that prescribed treatments or services for Medicaid and Medicare members are pre-approved to meet the insurer's requirements. By meticulously detailing the necessary member information, including plan type, member ID, and contact details, this form initiates the process of securing authorization for a wide array of services ranging from elective or routine to expedited or urgent, the latter being defined as services required to prevent serious health deterioration or loss of functional capacity. It encompasses a broad spectrum of healthcare needs, including inpatient and outpatient services, surgical procedures, diagnostics, rehabilitative care, and more, mandating specific information about the provider, service type, and anticipated healthcare interventions. The form further requires diagnostic codes, procedure descriptions, and a detailed account of the proposed service dates and frequencies, underscoring the importance of precision in the prior authorization process. With designated sections for clinical notes and supporting documentation, the form facilitates a comprehensive review by Molina Healthcare, guided by the principle that thorough preparation and clear communication are vital to expediting the approval process and ensuring timely access to necessary medical care.
| Question | Answer |
|---|---|
| Form Name | Michigan Molina Prior Authorization Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | molina medicaid prior authorization form michigan, molina prior authorization form michigan, molina prior authorization form pdf, molina prior authorization form for medication |
Molina Healthcare of Michigan Prior Authorization Request Form
Phone Number: (888)
Medicaid Fax Number: (800)
Medicare Fax: (888)
Member I nformat ion
Plan: |
Molina Medicaid |
Member Name:
Molina MI Child
Molina Medicare
DOB:
Other:
Member I D# : |
|
Member Phone # : |
( |
) |
Service I s:
Elective/ Routine
Expedited/ Urgent *
*Definition of Urgent / Expedited service request designation is w hen the treat ment requested is required to prevent serious deterioration in the member’s health or could jeopardize the member’s ability to regain maximum function. Requests outside of this definition should be submitted as routine/ non- urgent.
Referral/ Service Type Request ed
|
I npatient |
|
|
|
|
|
|
Outpatient |
|
|
|
||||||
|
Surgical Procedures |
|
|
|
|
|
|
Surgical Procedure |
|
DME |
|
||||||
|
ED Admission |
|
|
|
|
|
|
Rehab (PT, OT, & ST) |
|
|
|
||||||
|
Direct Admission |
|
|
|
|
|
|
Diagnostic Procedure |
|
|
|
||||||
|
SNF |
|
|
|
|
|
|
I maging |
|
Home Health |
|
||||||
|
Rehab |
|
|
|
|
|
|
Chiropractic |
|
|
|
||||||
|
LTAC |
|
|
|
|
|
|
Wound Care |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
I nfusion Therapy |
|
I n Office |
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Referred To Provider/ Facility Name & Tax I D# : _____ |
|
|
|
|||||||||||||
|
Referred To Address & Phone# : |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Diagnosis Code & Description: |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
CPT/ HCPCS Code & Description: |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Number of visits requested: |
|
|
|
|
|
Date(s) of Service: |
|
|
|
|||||||
|
|
Please send clinical not es and any support ing document at ion |
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
Provider I nformat ion |
|
|
|
||||
|
Requesting Provider Name and Address: |
|
|
|
|||||||||||||
|
Contact @ Requesting Provider’s: |
|
|
|
|
|
|
|
|
|
|
||||||
|
Phone Number: ( |
) |
|
|
|
|
|
|
|
|
Fax Number: ( |
) |
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For Molina Use Only: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2013 MI Molina Healthcare/ Molina Medicare PA GUI DE 5/ 8/ 13