
You may prepare Mltc 62 Form instantly by using our online tool for PDF editing. To maintain our tool on the leading edge of practicality, we aim to implement user-driven capabilities and enhancements regularly. We're always thankful for any suggestions - join us in revampimg PDF editing. By taking several simple steps, it is possible to start your PDF editing:
Step 1: Hit the orange "Get Form" button above. It is going to open our editor so you can begin filling in your form.
Step 2: With the help of our online PDF editor, you can accomplish more than merely fill in blanks. Express yourself and make your forms appear professional with custom text added in, or fine-tune the original content to excellence - all that comes with the capability to add your own graphics and sign the PDF off.
Pay close attention while filling in this pdf. Make sure every single blank field is filled in accurately.
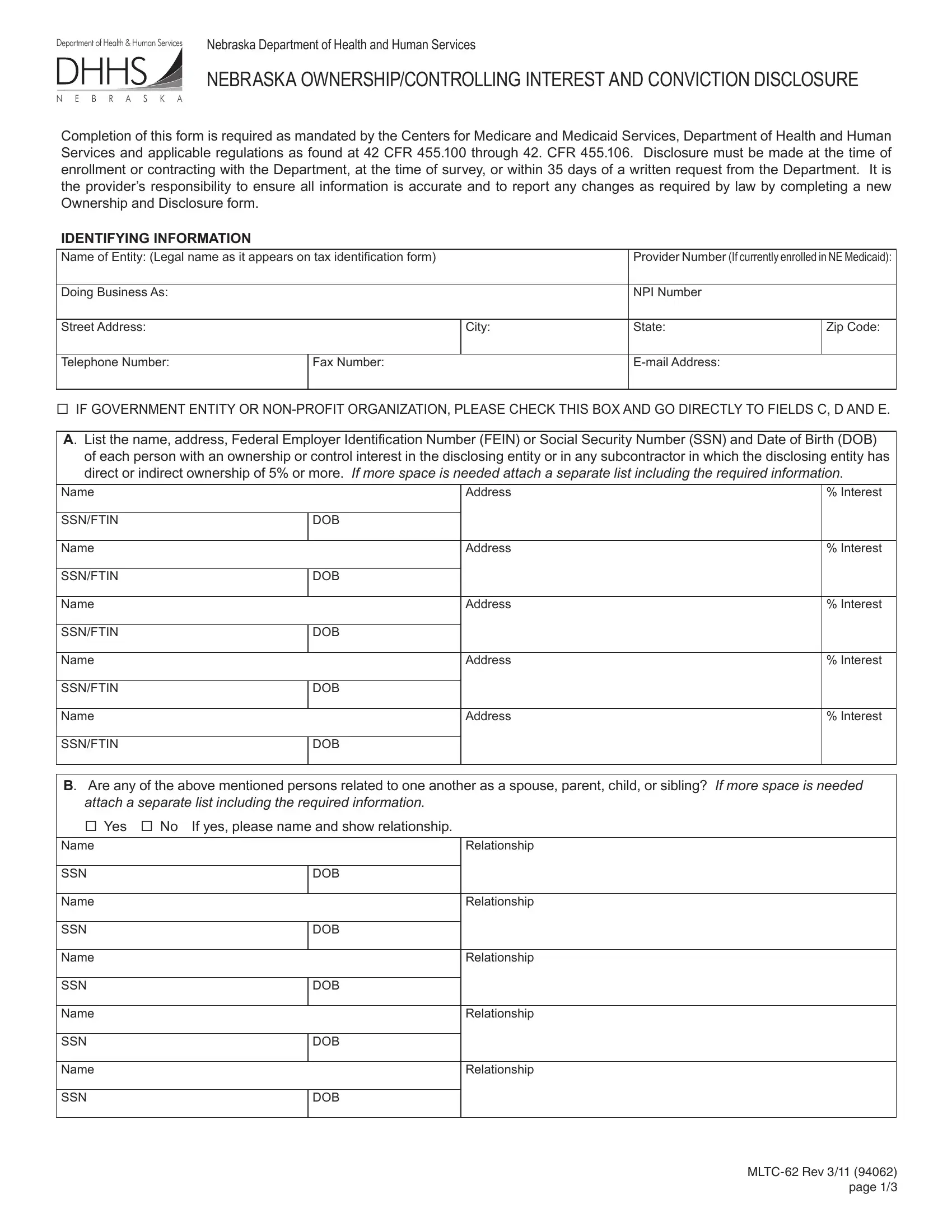
1. Start completing the Mltc 62 Form with a group of essential blanks. Consider all of the important information and be sure nothing is missed!
2. Once your current task is complete, take the next step – fill out all of these fields - SSNFTIN, Name, SSNFTIN, Address, DOB, DOB, Interest, B Are any of the above mentioned, attach a separate list including, If yes please name and show, Name, SSN, Name, SSN, and Name with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
3. This third section should be pretty uncomplicated, Name, SSN, Relationship, DOB, and MLTC Rev page - all these blanks must be filled out here.

4. This next section requires some additional information. Ensure you complete all the necessary fields - If more space is needed attach a, Name, SSN, Name, SSN, Name, SSN, Name, SSN, Name, SSN, Name, SSN, Position Title, and Position Title - to proceed further in your process!
5. Now, the following final part is precisely what you should finish prior to submitting the document. The fields here include the next: Name, SSNFTIN, Name, SSNFTIN, Name, SSNFTIN, Other Provider Name, Other Provider Name, Other Provider Name, DOB, DOB, DOB, Interest, Interest, and Interest.
Always be extremely mindful while filling out Name and SSNFTIN, because this is where many people make a few mistakes.
Step 3: Ensure that your information is correct and just click "Done" to proceed further. Make a 7-day free trial account with us and get immediate access to Mltc 62 Form - which you can then use as you want inside your FormsPal cabinet. When using FormsPal, you'll be able to complete documents without being concerned about personal data incidents or records getting shared. Our secure software ensures that your personal information is stored safely.