Are you an existing Molina Healthcare member having issues with resolution requests? We understand that it can be frustrating trying to get the help you need when dealing with insurance. In this blog post, we'll discuss the Molina Healthcare Resolution Request Form and how it can help streamline your health care experience and make sure you're getting the coverage and support you deserve. We'll go over important details like eligibility requirements, instructions on how to submit a request, where to find helpful resources, as well as tips on what not to include in your form submission and more. Keep reading to learn more about the recent changes regarding resolution requests and start taking control of your healthcare today!
| Question | Answer |
|---|---|
| Form Name | Molina Healthcare Resolution Request Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | molina dispute form florida pdf, molina appeal form, molina dispute resolution request form, molina provider dispute resolution request |
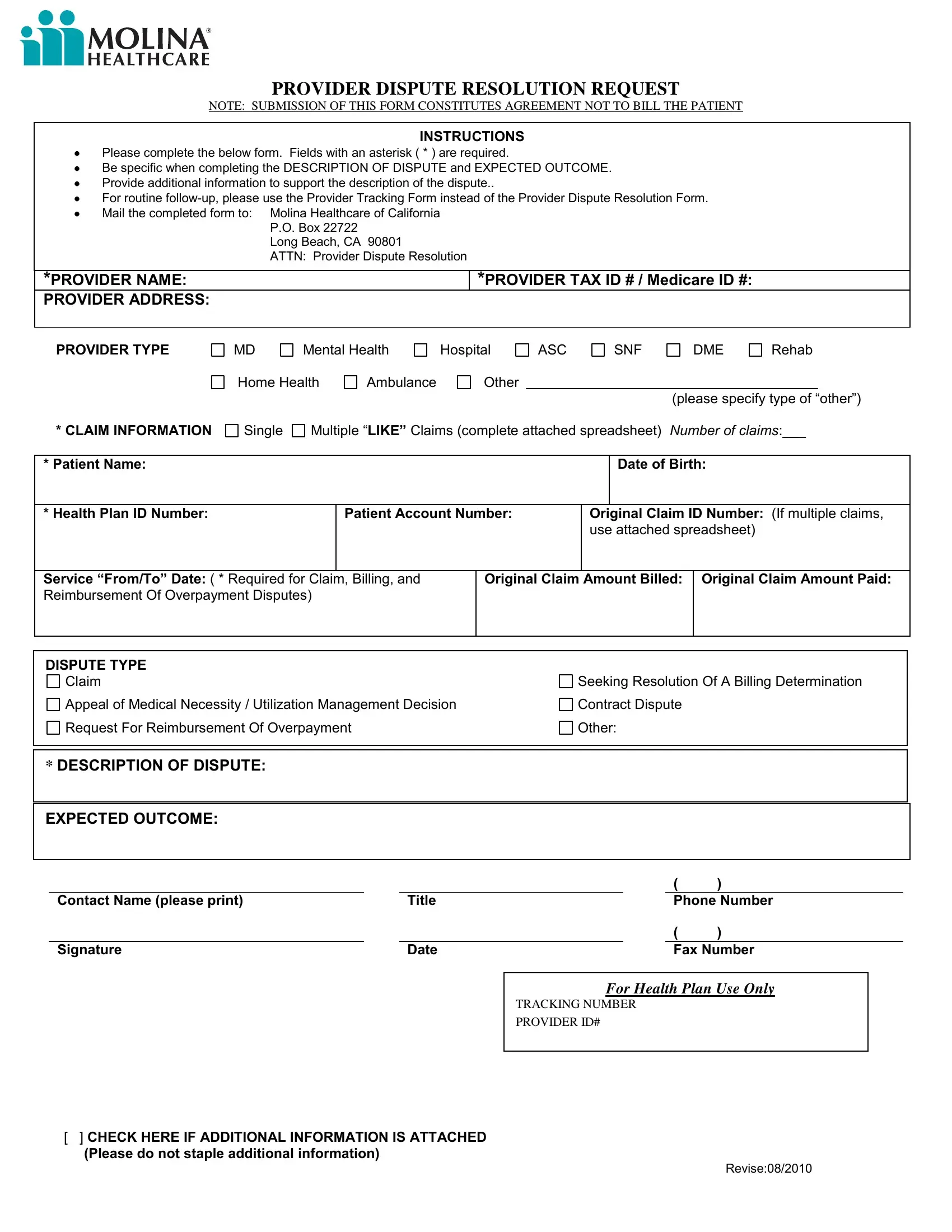
PROVIDER DISPUTE RESOLUTION REQUEST
NOTE: SUBMISSION OF THIS FORM CONSTITUTES AGREEMENT NOT TO BILL THE PATIENT
INSTRUCTIONS
Please complete the below form. Fields with an asterisk ( * ) are required.
Be specific when completing the DESCRIPTION OF DISPUTE and EXPECTED OUTCOME.
Provide additional information to support the description of the dispute..
For routine
Mail the completed form to: |
Molina Healthcare of California |
|
|
P.O. Box 22722 |
|
|
Long Beach, CA 90801 |
|
|
ATTN: Provider Dispute Resolution |
|
|
|
|
*PROVIDER NAME: |
|
*PROVIDER TAX ID # / Medicare ID #: |
PROVIDER ADDRESS: |
|
|
|
|
|
PROVIDER TYPE
* CLAIM INFORMATION
MD |
Mental Health |
Hospital |
ASC |
SNF |
DME |
Rehab |
|
Home Health |
Ambulance |
Other |
|
|
|
|
|
(please specify type of “other”)
Single Multiple “LIKE” Claims (complete attached spreadsheet) NUMBER OF CLAIMS:___
* Patient Name:
Date of Birth:
* Health Plan ID Number: |
Patient Account Number: |
Original Claim ID Number: (If multiple claims, |
||
|
|
|
use attached spreadsheet) |
|
|
|
|
|
|
Service “From/To” Date: ( * Required for Claim, Billing, and |
Original Claim Amount Billed: |
Original Claim Amount Paid: |
||
Reimbursement Of Overpayment Disputes) |
|
|
|
|
|
|
|
|
|
DISPUTE TYPE
Claim
Appeal of Medical Necessity / Utilization Management Decision
Request For Reimbursement Of Overpayment
Seeking Resolution Of A Billing Determination Contract Dispute
Other:
*DESCRIPTION OF DISPUTE:
EXPECTED OUTCOME:
|
|
|
( |
) |
|
Contact Name (please print) |
|
Title |
|
Phone Number |
|
|
|
|
( |
) |
|
Signature |
|
Date |
|
Fax Number |
|
For Health Plan Use Only
TRACKING NUMBER
PROVIDER ID#
[] CHECK HERE IF ADDITIONAL INFORMATION IS ATTACHED (Please do not staple additional information)
Revise:08/2010