

It is possible to fill in msa 115 pdf effectively with the help of our PDFinity® editor. Our development team is always endeavoring to enhance the editor and insure that it is even faster for people with its extensive features. Take full advantage of present-day modern prospects, and discover a trove of new experiences! Starting is effortless! All you should do is take the following easy steps below:
Step 1: Simply hit the "Get Form Button" above on this page to access our pdf file editing tool. Here you'll find all that is required to work with your document.
Step 2: With our online PDF tool, you are able to accomplish more than merely fill out blank fields. Express yourself and make your docs seem great with customized text put in, or tweak the file's original input to perfection - all that comes with an ability to add any type of graphics and sign the PDF off.
This PDF doc will require some specific information; in order to guarantee correctness, please make sure to heed the next suggestions:
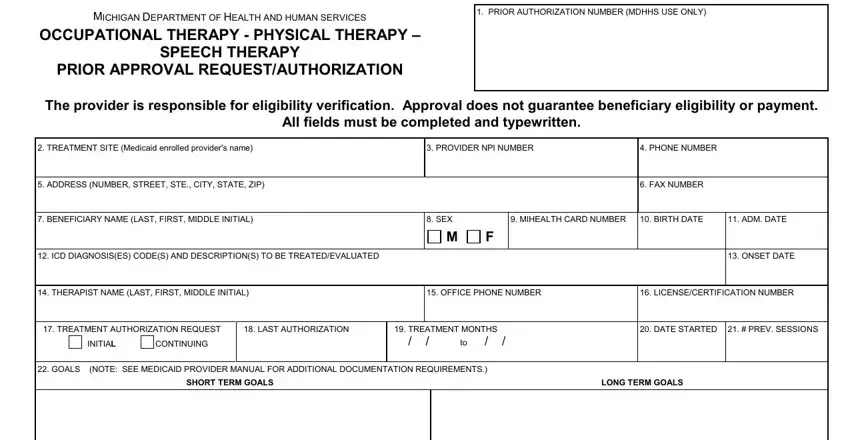
1. It's essential to fill out the msa 115 pdf correctly, so take care when filling out the segments comprising these particular fields:
2. The next step is to complete the following blanks: PROGRESS SUMMARY NOTE SEE, SCHOOL THERAPY PROGRAMS NO, YES, TREATMENT REQUESTED FREQUENCY, LINE NO, PROCEDURE CODE, MODIFIER, TOTAL UNITS PER PA, MDHHS USE ONLY, AUTHORIZATION PERIOD APPROVED, REVIEW ACTION, APPROVED RETURNED DENIED NO ACTION, CONSULTANT REMARKS, See CHAMPS, and recertify.
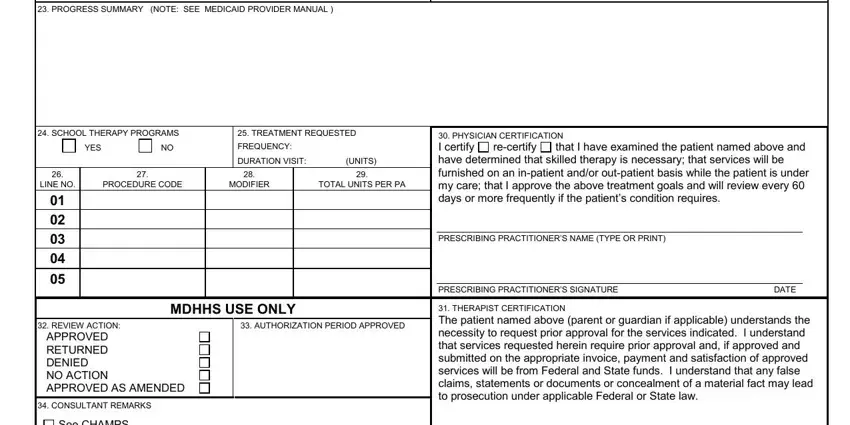
Be extremely mindful when filling in TOTAL UNITS PER PA and TREATMENT REQUESTED FREQUENCY, because this is the part in which many people make mistakes.
3. This next portion is mostly about See CHAMPS, THERAPIST CERTIFICATION The, CONSULTANT SIGNATURE, DATE, MSA Previous editions are obsolete, and Page of - fill out each one of these blank fields.

Step 3: You should make sure the details are correct and then click "Done" to progress further. Sign up with us right now and instantly get access to msa 115 pdf, prepared for downloading. Each and every edit made is handily preserved , making it possible to modify the document at a later stage if necessary. FormsPal guarantees protected document tools without data recording or sharing. Feel safe knowing that your details are safe with us!