
With the help of the online PDF tool by FormsPal, you can easily fill out or change eligibility here. To retain our editor on the cutting edge of efficiency, we work to implement user-oriented features and improvements regularly. We're routinely glad to get feedback - help us with revampimg PDF editing. With just several simple steps, you'll be able to start your PDF editing:
Step 1: Simply click on the "Get Form Button" above on this page to see our pdf file editing tool. This way, you will find all that is needed to fill out your document.
Step 2: This tool lets you work with PDF documents in many different ways. Transform it by writing your own text, adjust existing content, and add a signature - all within the reach of several mouse clicks!
This form will require you to enter specific details; to ensure accuracy, be sure to take into account the following steps:
1. Fill out your eligibility with a number of essential blanks. Gather all of the necessary information and make sure absolutely nothing is neglected!
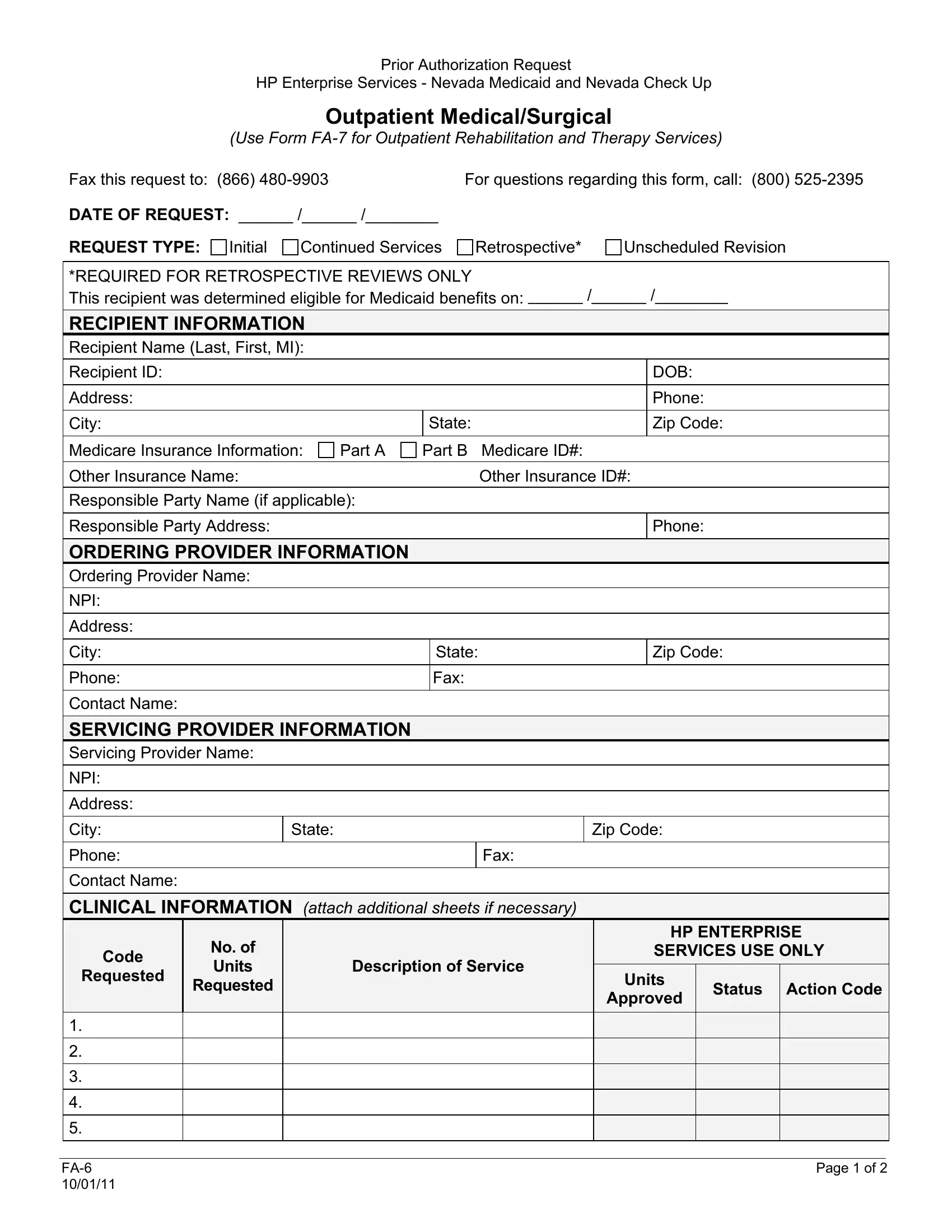
2. When the previous part is complete, you're ready put in the essential details in DATE OF REQUEST REQUEST TYPE, Zip Code, State, State, Zip Code, Code, Requested, No of Units, Requested, Description of Service, HP ENTERPRISE, SERVICES USE ONLY Units, Status Action Code, and Approved allowing you to go further.
3. Through this stage, take a look at Requested, Status Action Code, Approved, and Page of. Every one of these are required to be taken care of with utmost precision.

Always be very mindful while completing Requested and Status Action Code, since this is the part in which most users make errors.
4. The next part will require your attention in the following areas: Use Form FA for Outpatient, No Yes, and Is the service you are requesting. Always enter all needed information to go onward.
5. The pdf needs to be concluded by dealing with this segment. Further you can see a full list of fields that need accurate information to allow your document usage to be accomplished: Is the service you are requesting, and Approved Through Denied Through.
Step 3: After you have looked once again at the information in the file's blanks, click on "Done" to complete your form at FormsPal. Get hold of the eligibility after you sign up at FormsPal for a 7-day free trial. Immediately access the pdf form in your FormsPal account, together with any modifications and changes conveniently saved! FormsPal guarantees risk-free document editing devoid of data record-keeping or sharing. Rest assured that your details are in good hands here!