
Handling PDF forms online is certainly super easy with this PDF editor. You can fill in New Hampshire Form 2620 here effortlessly. In order to make our tool better and more convenient to work with, we constantly implement new features, taking into consideration feedback from our users. To get the ball rolling, take these simple steps:
Step 1: Click on the orange "Get Form" button above. It will open up our pdf tool so you could start completing your form.
Step 2: This editor helps you change nearly all PDF forms in many different ways. Enhance it by adding your own text, adjust what's already in the file, and place in a signature - all at your fingertips!
Be attentive while filling out this pdf. Make sure that every blank field is done accurately.
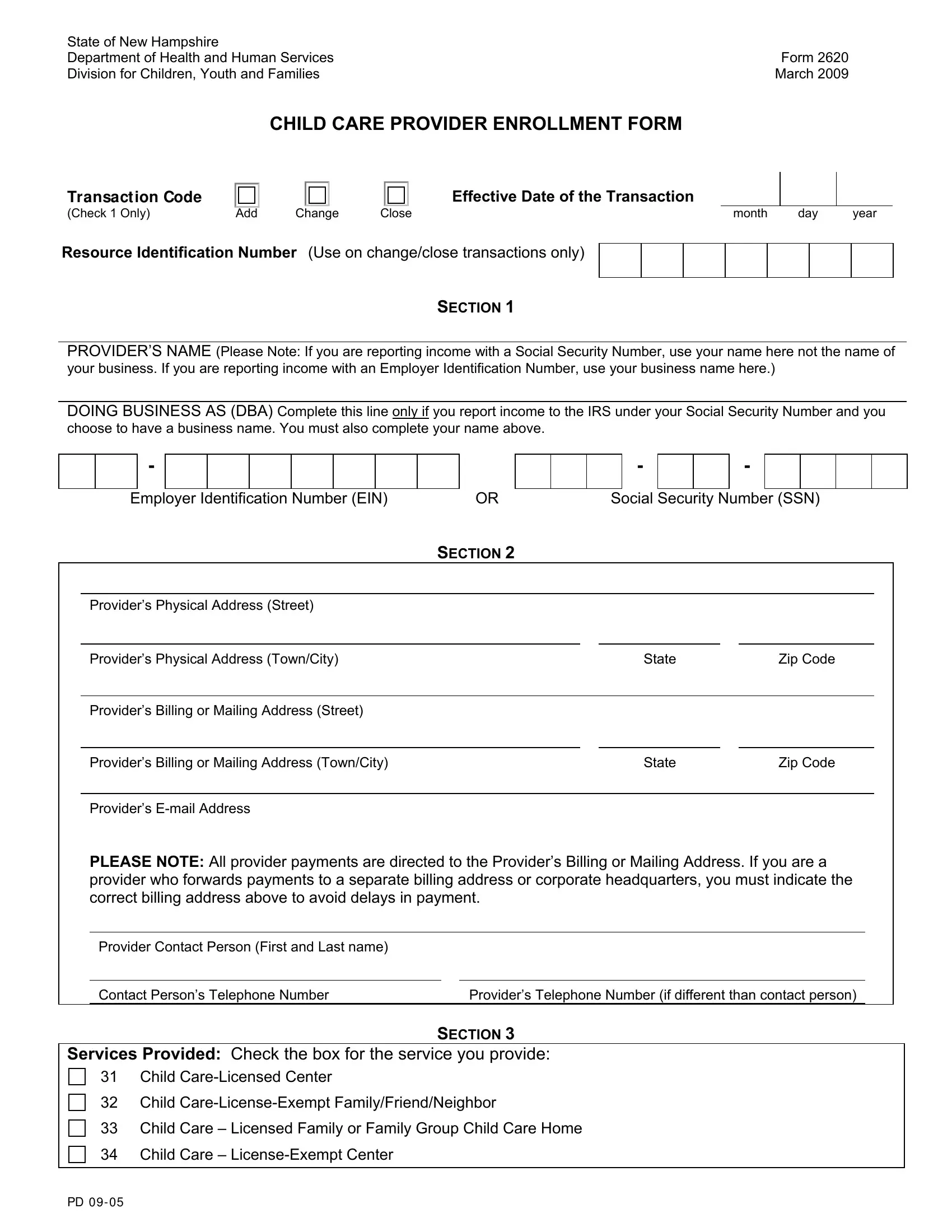
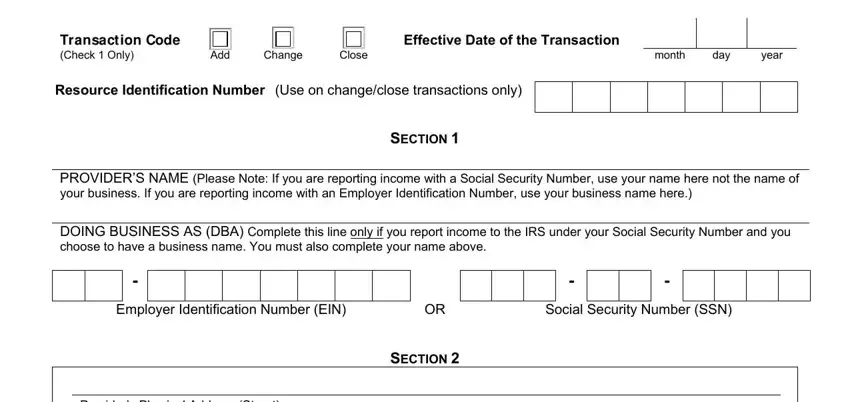
1. First of all, while completing the New Hampshire Form 2620, begin with the page that has the following blanks:
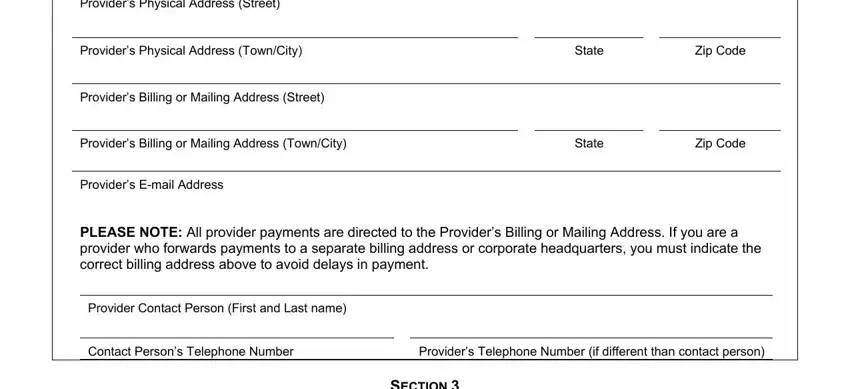
2. When the prior section is filled out, go to type in the suitable details in these - Providers Physical Address Street, Providers Physical Address TownCity, Providers Billing or Mailing, Providers Billing or Mailing, Providers Email Address, State, State, Zip Code, Zip Code, PLEASE NOTE All provider payments, Provider Contact Person First and, Providers Telephone Number if, and SECTION.
3. This next step focuses on Services Provided Check the box, Child CareLicensed Center, Child CareLicenseExempt, Child Care Licensed Family or, and Child Care LicenseExempt Center - fill out these fields.

As to Child Care LicenseExempt Center and Services Provided Check the box, make sure you don't make any mistakes here. Those two could be the key fields in this PDF.
Step 3: Check the information you've entered into the blank fields and then click on the "Done" button. Obtain your New Hampshire Form 2620 the instant you sign up for a free trial. Easily view the pdf document inside your personal account page, together with any edits and adjustments automatically saved! At FormsPal, we strive to be certain that your information is maintained private.