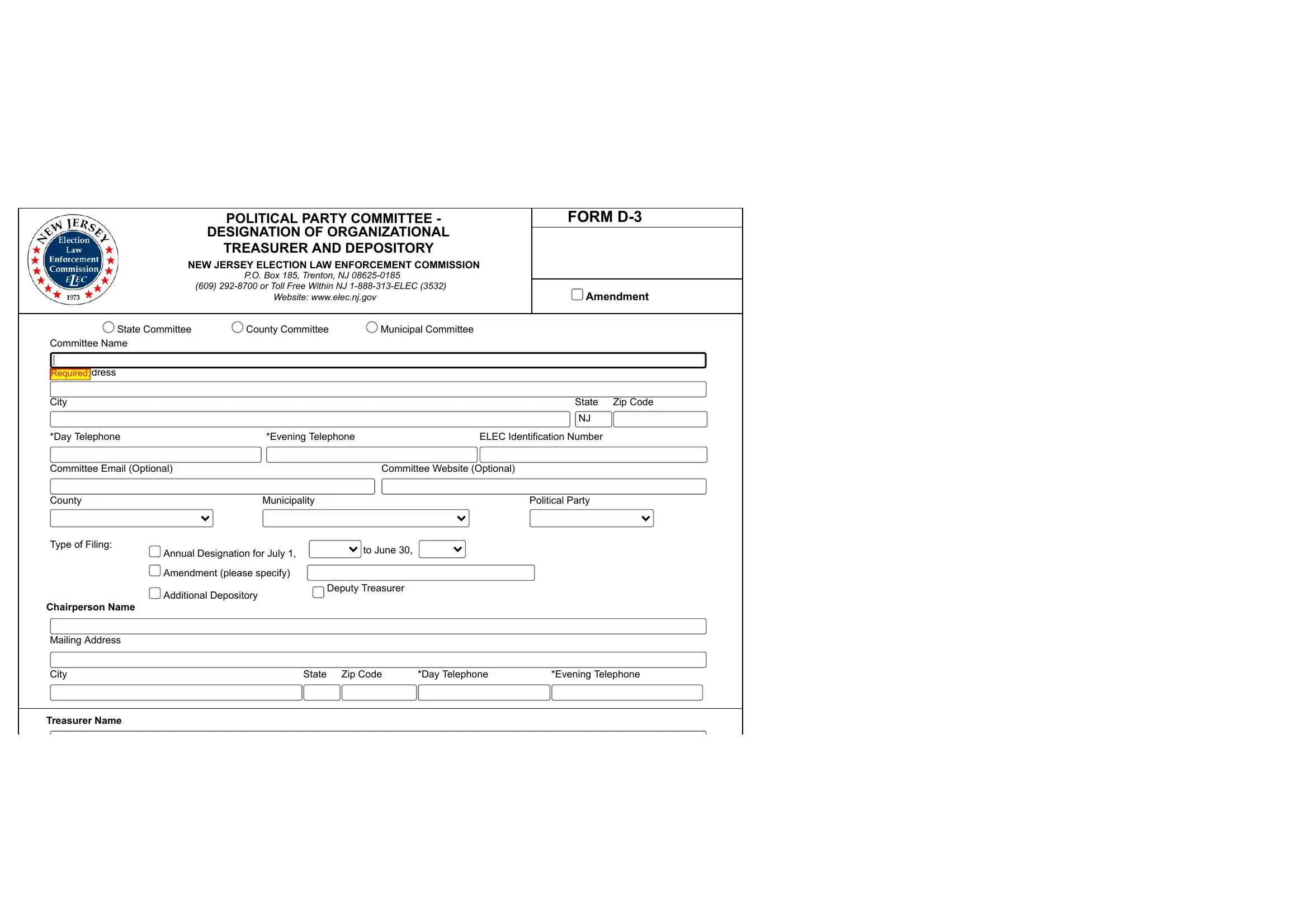
Are you planning to launch a new business in New Jersey? If so, then you might be familiar with the term "Form D 3," which is essentially an organizational structure that is used by businesses in order to secure state approval for their operations. Form D 3 requires that companies submit certain documents proving their compliance with state requirements and enabling states to regulate them going forward - making it a crucial element of starting up in New Jersey. In this blog post, we'll cover all the details surrounding Form D 3 and the steps needed to effectively complete and submit it, giving entrepreneurs greater peace of mind when venturing into uncharted waters. So read on if you're serious about launching your business soon!
| Question | Answer |
|---|---|
| Form Name | New Jersey Form D 3 |
| Form Length | 4 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min |
| Other names | 1-888-313-ELEC, New_Jersey, 1A-1, nj elec forms |

POLITICAL PARTY COMMITTEE - DESIGNATION OF |
FORM |
|||||
ORGANIZATIONAL TREASURER AND DEPOSITORY |
FOR STATE USE ONLY |
|||||
|
|
|||||
NEW JERSEY ELECTION LAW ENFORCEMENT COMMISSION |
|
|
||||
|
P.O. Box 185, Trenton, NJ |
|
|
|||
|
(609) |
|
|
|||
|
www.elec.state.nj.us/ |
|
|
|
||
|
|
|
|
|
|
|
PLEASE TYPE OR PRINT |
|
|
|
|
|
|
|
|
|
|
|
|
|
Committee Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
State Committee |
County Committee |
Municipal Committee |
|
|
||
|
|
|
|
|
|
|
Address (Number and Street, City, State, Zip Code) |
|
|
|
|
|
|
|
|
|
|
|
|
|
*(Area) Day Telephone |
|
|
|
*(Area) Evening Telephone |
|
|
|
|
|
|
|
|
|
County |
|
|
|
Municipality |
|
|
|
|
|
|
|
|
|
ELEC Identification Number |
|
|
|
Political Party |
|
|
|
|
|
|
|
||
Annual Designation for July 1, ________ to June 30, ________ |
Additional Depository |
Deputy Treasurer |
||||
Amendment (please specify) __________________________________________________________________________ |
||||||
|
|
|
|
|
|
|
1. CHAIRPERSON |
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
|
Zip Code |
|
|
|
|
|
|
|
*(Area) Day Telephone |
|
|
|
*(Area) Evening Telephone |
|
|
|
|
|
|
|
|
|
2. TREASURER |
|
|
|
|
|
|
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
|
Zip Code |
|
|
|
|
|
|
|
*(Area) Day Telephone |
|
|
|
*(Area) Evening Telephone |
|
|
|
|
|
|
|
|
|
Resident Address, if different from Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
|
Zip Code |
|
|
|
|
|
|
|
3. DEPOSITORY INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Bank or Depository |
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
City |
|
|
|
State |
|
Zip Code |
|
|
|
|
|
|
|
(Area) Day Telephone |
|
|
|
|
|
|
|
|
|
|
|
|
|
Account Name |
|
|
|
Account Number |
|
|
|
|
|
|
|
|
|
New Jersey Election Law Enforcement Commission |
Form |
*Leave this field blank if your telephone number is unlisted. Pursuant |
to N.J.S.A. |
|
Page 1 of 2 |
3. DEPOSITORY INFORMATION
Name of Bank or Depository
Mailing Address
City |
State |
|
Zip Code |
|
|
|
|
(Area) Day Telephone |
|
|
|
|
|
|
|
Account Name |
Account Number |
|
|
|
|
|
|
LIST THE NAME(S), MAILING ADDRESS(ES) AND TELEPHONE NUMBER(S) OF ANY PERSON(S) AUTHORIZED TO |
|||
SIGN CHECKS OR OTHERWISE MAKE TRANSACTIONS |
|
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
City |
State |
|
Zip Code |
|
|
|
|
*(Area) Day Telephone |
*(Area) Evening Telephone |
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
City |
State |
|
Zip Code |
|
|
|
|
*(Area) Day Telephone |
*(Area) Evening Telephone |
|
|
|
|
|
|
Name |
|
|
|
|
|
|
|
Mailing Address |
|
|
|
|
|
|
|
City |
State |
|
Zip Code |
|
|
|
|
*(Area) Day Telephone |
*(Area) Evening Telephone |
|
|
|
|
|
|
TREASURER /CHAIRPERSON CERTIFICATION
I certify that the statements on this document are true. I am aware that if any of the statements are willfully false, I may be subject to punishment.
_______________________ |
______________________________________ |
_____________________________________ |
DATE |
PRINT FULL NAME (TREASURER) |
SIGNATURE (TREASURER) |
_______________________ |
______________________________________ |
_____________________________________ |
DATE |
PRINT FULL NAME (CHAIRPERSON) |
SIGNATURE (CHAIRPERSON) |
Treasurers for the State Political Party Committees are required to receive training with the New Jersey Election Law Enforcement Commission.
Check here if you have completed the training and enter your Treasurer Training ID#______________________.
New Jersey Election Law Enforcement CommissionForm D3 Revised: 02/2011
*Leave this field blank if your telephone number is unlisted. Pursuant to N.J.S.A.