In the heart of New Mexico's efforts to support the nutritional needs of infants, children, and women under the Women, Infants & Children (WIC) program, lies the New Mexico WIC Medical Request for Formula/Food form. This document facilitates the provision of essential formula and food to those who have specific medical needs or conditions that regular WIC offerings cannot meet, ensuring that every beneficiary receives tailored nutritional support. The form requires detailed patient information, including the name, date of birth, and medical diagnosis coded per the International Classification of Diseases (ICD-9), which underscores the medical necessity for special formulas or foods. Notably, the form lists a broad spectrum of conditions, such as allergies, autoimmune disorders, and various other health issues that can affect nutritional intake and growth. The healthcare provider's endorsement, essentially through their signature, mandates a careful consideration of each request, abiding by program policies and conditions that underscore the safety and well-being of the participants. Section B of the form delineates the formula or food requested, including the amount and duration of the supply, demonstrating the program's adaptability to the specific nutritional needs and medical conditions of its participants. Moreover, it highlights the federal guidelines that cap the provision to a maximum allowed by law unless a greater need is indicated, showcasing the balance between individual care and regulatory compliance. Additionally, with a nod to inclusivity and anti-discrimination, the form concludes with a statement aligning with federal law and USDA policy, ensuring equal opportunity and provision for all eligible individuals regardless of race, color, national origin, sex, age, or disability, cementing the form's role not just in nutrition but in upholding principles of equity and justice.
| Question | Answer |
|---|---|
| Form Name | New Mexico Wic Prescription Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | Pediasure, Gerber, New_Mexico, wic prescription formula nm printablw |
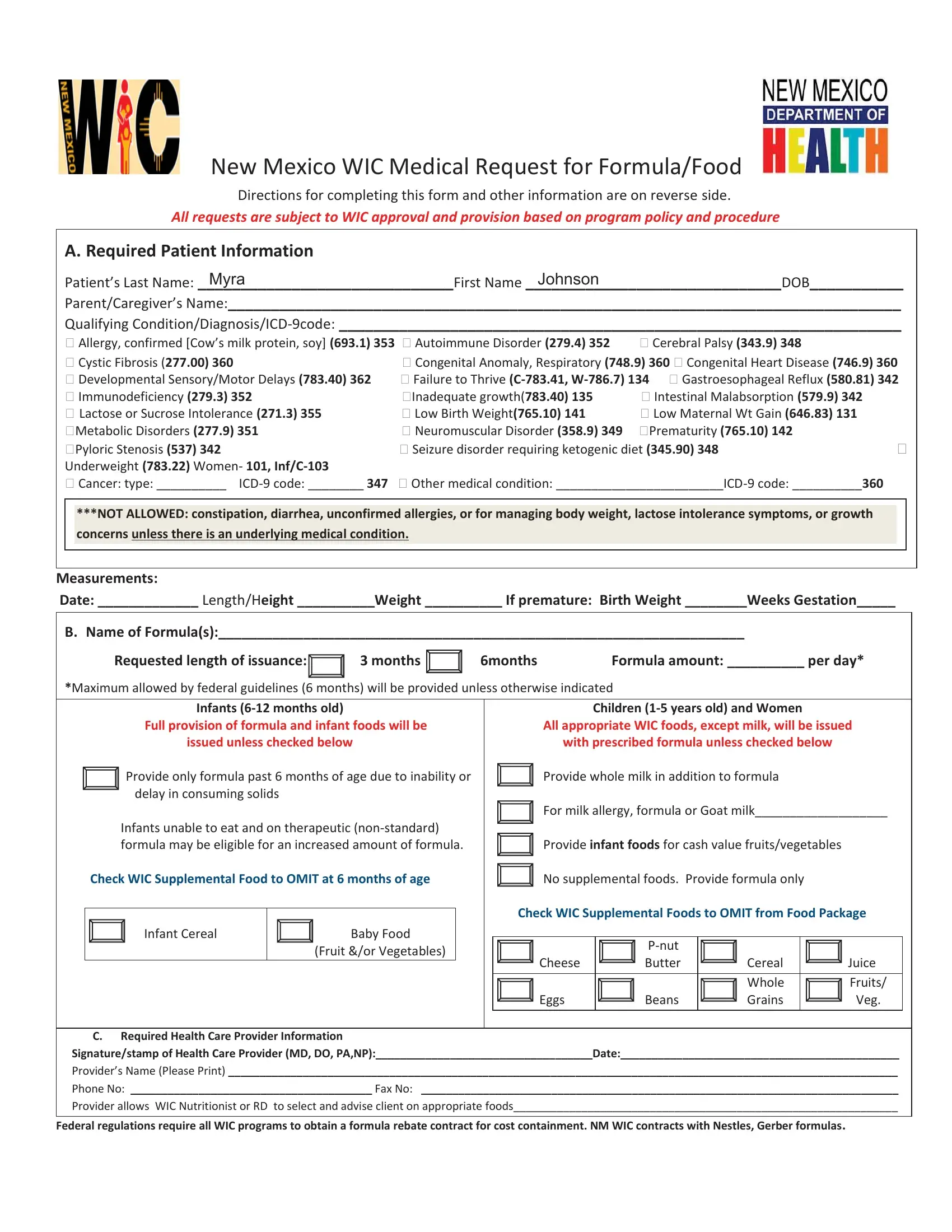
New Mexico WIC Medical Request for Formula/Food
Directions for completing this form and other information are on reverse side.
All requests are subject to WIC approval and provision based on program policy and procedure
|
A. Required Patient Information |
|
|
|
|
|
|
|
|
|
|
Patient’s Last Name: MYRA |
|
|
First Name |
JOHNSON |
DOB___________ |
||||
|
Parent/Caregiver’s Name:_______________________________________________________________________________ |
|||||||||
|
Qualifying |
|||||||||
|
Allergy, confirmed [Cow’s milk protein, soy] (693.1) 353 Autoimmune Disorder (279.4) 352 |
Cerebral Palsy (343.9) 348 |
|
|
|
|||||
|
Cystic Fibrosis (277.00) 360 |
|
Congenital Anomaly, Respiratory (748.9) 360 Congenital Heart Disease (746.9) 360 |
|||||||
|
Developmental Sensory/Motor Delays (783.40) 362 |
Failure to Thrive |
||||||||
|
Immunodeficiency (279.3) 352 |
|
Inadequate growth(783.40) 135 |
Intestinal Malabsorption (579.9) 342 |
|
|
|
|||
|
Lactose or Sucrose Intolerance (271.3) 355 |
|
Low Birth Weight(765.10) 141 |
Low Maternal Wt Gain (646.83) 131 |
|
|
|
|||
|
Metabolic Disorders (277.9) 351 |
|
Neuromuscular Disorder (358.9) 349 |
Prematurity (765.10) 142 |
|
|
|
|||
|
Pyloric Stenosis (537) 342 |
|
Seizure disorder requiring ketogenic diet (345.90) 348 |
|||||||
|
Underweight (783.22) Women- 101, |
|
|
|
|
|
|
|
|
|
|
Cancer: type: __________ |
Other medical condition: |
|
|
|
|||||
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|||||
|
|
***NOT ALLOWED: constipation, diarrhea, unconfirmed allergies, or for managing body weight, lactose intolerance symptoms, or growth |
|
|
|
|||||
|
|
concerns unless there is an underlying medical condition. |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Measurements: |
|
|
|
|
|
|
|
|
||
Date: _____________ Length/Height __________Weight __________ If premature: Birth Weight ________Weeks Gestation_____ |
|
|
|
|||||||
|
|
|
|
|
|
|||||
|
B. Name of Formula(s):____________________________________________________________________ |
|
|
|
||||||
|
|
Requested length of issuance: |
3 months |
6months |
Formula amount: __________ per day* |
|
|
|
||
|
*Maximum allowed by federal guidelines (6 months) will be provided unless otherwise indicated |
|
|
|
|
|||||
Infants
Full provision of formula and infant foods will be issued unless checked below
Provide only formula past 6 months of age due to inability or delay in consuming solids
Infants unable to eat and on therapeutic
Check WIC Supplemental Food to OMIT at 6 months of age
Infant Cereal |
Baby Food |
|
(Fruit &/or Vegetables) |
Children
All appropriate WIC foods, except milk, will be issued
with prescribed formula unless checked below
Provide whole milk in addition to formula
For milk allergy, formula or Goat milk___________________
Provide infant foods for cash value fruits/vegetables
No supplemental foods. Provide formula only
Check WIC Supplemental Foods to OMIT from Food Package
|
|
|
|
Cheese |
Butter |
Cereal |
Juice |
|
|
Whole |
Fruits/ |
Eggs |
Beans |
Grains |
Veg. |
C.Required Health Care Provider Information
Signature/stamp of Health Care Provider (MD, DO, PA,NP):___________________________________Date:_____________________________________________
Provider’s Name (Please Print) ____________________________________________________________________________________________________________
Phone No: _______________________________________ Fax No: _____________________________________________________________________________
Provider allows WIC Nutritionist or RD to select and advise client on appropriate foods______________________________________________________________
Federal regulations require all WIC programs to obtain a formula rebate contract for cost containment. NM WIC contracts with Nestles, Gerber formulas.

|
New Mexico Medical Request for Formula/Food |
Directions: |
For ALL PATIENTS: Complete Sections A |
|
For MEDICAL FORMULA AND FOOD: Complete Section B |
|
For HEALTH CARE PROVIDER SIGNATURE: Complete Section C |
Please return this form to participant’s WIC clinic. (FAX is acceptable)
The following formulas are available from NM WIC (Women, Infants & Children)
|
Star Medical Issued Formula |
Standard |
NO RX Needed |
|
|
|
(Infants & Children) |
|
(Women, Infants & Children) |
for Infants under |
|
|
|
|
|
12 mo |
|
|
Boost Kid Essentials 1.0 8oz (children) |
Alimentum powder 16oz 22 cal/per/oz (infants/children) |
|
|
|
|
Boost Kid Essentials 1.5 8oz (children) |
Alimentum RTF 32oz (infants/children) |
|
|
|
|
Boost Kid Essentials 1.5 w/fiber 8oz (children) |
Boost Kid Essentials 8.25oz – van/choc (children) |
|
|
|
|
|
|
|
|
|
|
Bright Beginnings Soy RTF 8 oz (children) |
Boost Plus RTF 8oz (women and children) |
|
|
|
|
|
|
|
|
|
|
Elecare DHA/ARA 14.1 oz powder (infants/child) |
Enfacare powder 12.8oz 22 cal/per/oz (infants/children) |
|
|
|
|
|
|
|
|
|
|
Elecare Jr. Vanilla/plain powder 14.1oz |
Ensure RTF 8oz (women) |
|
|
|
|
(children) |
|
|
|
|
|
|
|
|
|
|
|
Enfacare RTF 32oz 22 cal/per/oz |
Gerber GS Gentle powder 12.7 oz (infant/child) |
X |
|
|
|
(infants/children) |
|
|
|
|
|
Enfamil Enfaport RTF 6 oz (infants) |
Gerber GS Gentle Conc. 12.1 oz (infant/child) |
X |
|
|
|
Enfamil Premature 24 cal 2 oz RTF |
Gerber GS Gentle RTF 8.45 oz 4pk( infant/child) |
X |
|
|
|
(infants/child) |
|
|
|
|
|
Enfamil Premature Hi Pro 24 cal 2oz RTF |
Gerber Good Start Gentle for supplementing 12.4 oz |
X |
|
|
|
(infants) |
|
(inf/child) |
|
|
|
Gerber GS Premature 24 cal RTF 3oz (infants) |
Gerber Good Start Soothe powder 12.4 oz (inf/child) |
X |
|
|
|
Hominex 1 powder 14.1oz (infants/children) |
Gerber Good Start Soy powder 12.9 oz (infant/child) |
X |
|
|
|
Hominex 2 powder 14.1 oz(Children) |
Gerber Good Start Soy Concentrate 12.1 oz (infant/child) |
X |
|
|
|
Ketocal 4:1 RTF (children) |
Gerber Good Start Soy RTF 8.45 oz 4 pk (infant/child) |
X |
|
|
|
Monogen powder 14.3oz (infants) |
Neosure Expert Care pwd 13.1 oz 22 cal (infant/child) |
|
|
|
|
Neocate DHA/ARA powder 14.1oz (infant/child) |
Nutramigen Enflora pwd 12.6 oz |
|
|
|
|
Neocate Jr powder 14oz (trop frt,choc,strawbry) |
Pediasure RTF 8 oz multiple flavors 6 pk(child) |
|
|
|
|
Neocate Jr. w/prebiotics 14oz Plain/Van (child) |
Pediasure w/fiber RTF 8 oz vanilla(child) |
|
|
|
|
Neosure RTF 32 oz 22 cal/per/oz (infants) |
Gerber Graduates Gentle Toddler pwd 22 oz (children) |
|
|
|
|
Nutramigen con. 13 oz (infants/children) |
Gerber Graduates Protect pwd 22 oz (children) |
|
|
|
|
|
|
|
|
|
|
Nutramigen RTF 32 oz (infants/children) |
Gerber Graduates Soy pwd 24 oz (children) |
|
|
|
|
|
|
|
|
|
|
Nutramigen Enflora LGG 12.6oz powder |
|
|
|
|
|
(children) |
|
|
|
|
|
Nutren Jr. 8.45 oz , Nutren Jr. 8.45 oz w/fiber |
|
|
|
|
|
Pediasure 1.5 RTF 8oz (children) |
|
|
|
|
|
Pediasure 1.5w/fiber RTF 8oz (children) |
|
|
|
|
|
Pediasure w/fiber ScFos Enteral 8oz RTF (child) |
|
|
|
|
|
Pediasure Peptide 1.5 8oz RTF (children) |
|
|
|
|
|
|
|
|
|
|
|
Neocate Splash 8oz RTF (children) |
|
|
|
|
|
|
|
|
|
|
|
Peptamen Jr. 1.0 RTF |
8.45oz Tetra pk (children) |
|
|
|
|
|
|
|
|
|
|
Peptamen Jr. 1.5 RTF |
8.45oz Tetra pk (children) |
|
|
|
|
|
|
|
|
|
|
Periflex powder 14 oz |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
Portagen powder 16 oz (infant/children) |
|
|
|
|
|
Pregestimil 16oz powder (infant/children) |
|
|
|
|
|
PurAmino powder 14.1oz (infants/children) |
|
|
|
|
|
Similac PM 60/40 powder (infant/children) |
Visit: www.nmwic.org for additional information. |
Rev. 2/2/2015 |
|
|
|
Similac Special Care 30cal 2oz RTF (infant) |
|
|
|
|
IN accordance with Federal law and U.S. Department of Agriculture policy, this institution is prohibited from discriminating on the basis of race, color, National origin, sex, age or disability. To file a complaint of discrimination, write USDA, Director, Office of Adjudication, 1400 Independence Ave. SW, Washington, D.C.