Are you interested in learning more about the New York Department of Insurance (DOI) requirements surrounding filing forms? If so, this blog post is a must read! Here, we’ll take an in-depth look at all that goes into filling out the necessary paperwork, including documents needed and consequences for incorrect or incomplete submissions. Whether you’re a newcomer to navigating DOI policy or need a refresher course on industry regulations, after reading this post you will have a complete understanding of what needs to be done when submitting information to the department. Let's get started!
| Question | Answer |
|---|---|
| Form Name | New York Dept Insurance Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | InsuranceCompla intForm state of new york dept of insurance form |

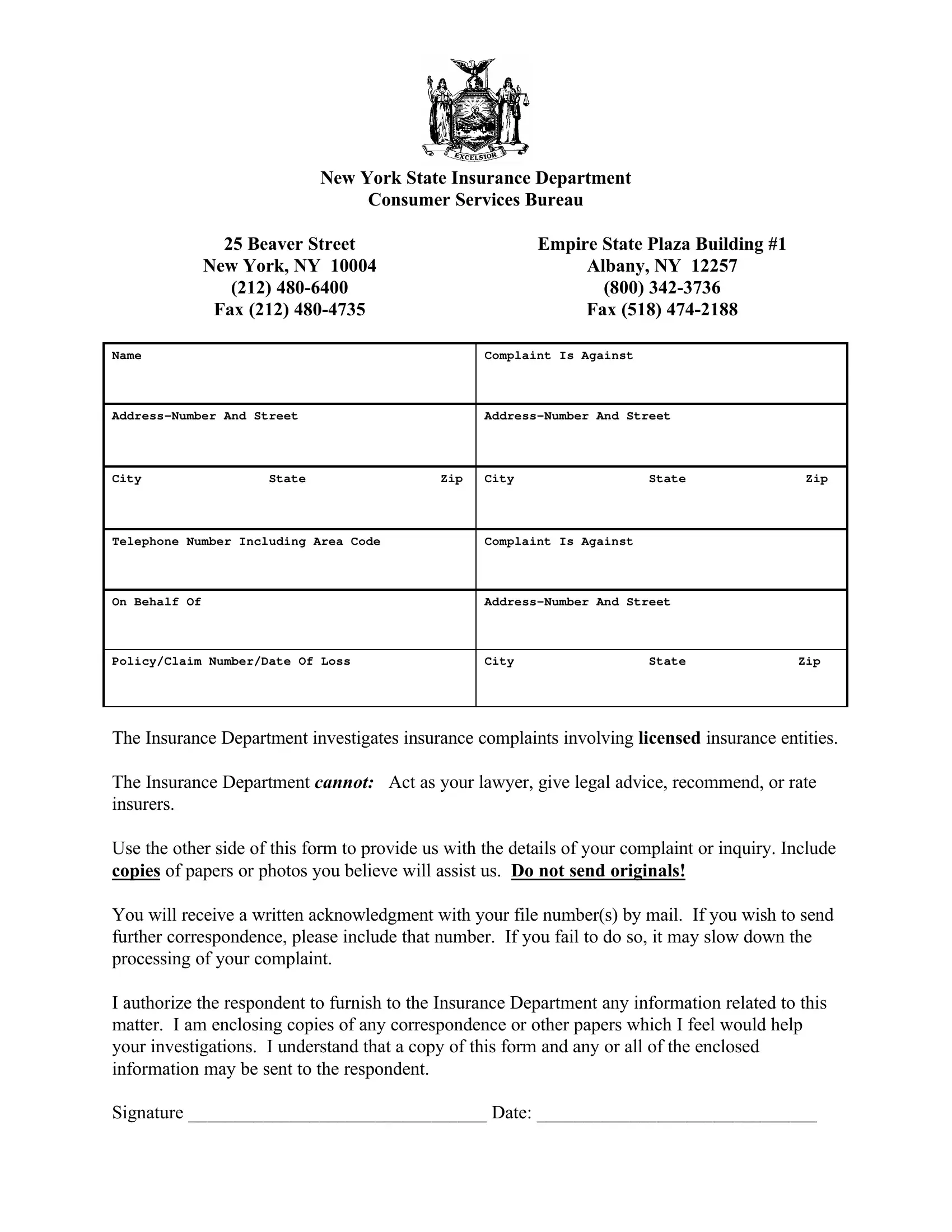
New York State Insurance Department
Consumer Services Bureau
|
25 Beaver Street |
|
|
Empire State Plaza Building #1 |
|
|
New York, NY 10004 |
|
|
Albany, NY 12257 |
|
|
(212) |
|
|
(800) |
|
|
Fax (212) |
|
|
Fax (518) |
|
|
|
|
|
|
|
Name |
|
|
Complaint Is Against |
|
|
|
|
|
|
||
|
|
||||
|
|
|
|
|
|
City |
State |
Zip |
City |
State |
Zip |
|
|
|
|
||
Telephone Number Including Area Code |
|
Complaint Is Against |
|
||
|
|
|
|
|
|
On Behalf Of |
|
|
|
||
|
|
|
|
|
|
Policy/Claim Number/Date Of Loss |
|
City |
State |
Zip |
|
|
|
|
|
|
|
The Insurance Department investigates insurance complaints involving licensed insurance entities.
The Insurance Department CANNOT: Act as your lawyer, give legal advice, recommend, or rate insurers.
Use the other side of this form to provide us with the details of your complaint or inquiry. Include copies of papers or photos you believe will assist us. Do not send originals!
You will receive a written acknowledgment with your file number(s) by mail. If you wish to send further correspondence, please include that number. If you fail to do so, it may slow down the processing of your complaint.
I authorize the respondent to furnish to the Insurance Department any information related to this matter. I am enclosing copies of any correspondence or other papers which I feel would help your investigations. I understand that a copy of this form and any or all of the enclosed information may be sent to the respondent.
Signature ________________________________ Date: ______________________________