Are you a New York resident who is about to conduct business in one of the five major agencies? If so, then you have likely heard about Form PS-409 – the form that serves as your agency’s statement of financial status. This helpful document outlines all methods and sources used for obtaining working capital, as well as other legal declarations regarding property ownership interests. By understanding the required information and purpose of this important form, you can ensure that your business dealings comply with state regulations. Read on to discover everything you need to know about filing Form PS-409 in New York.
| Question | Answer |
|---|---|
| Form Name | New York Form Ps 409 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | nys civil service forms ps 409, taxable, enrollees, ATTESTATION |
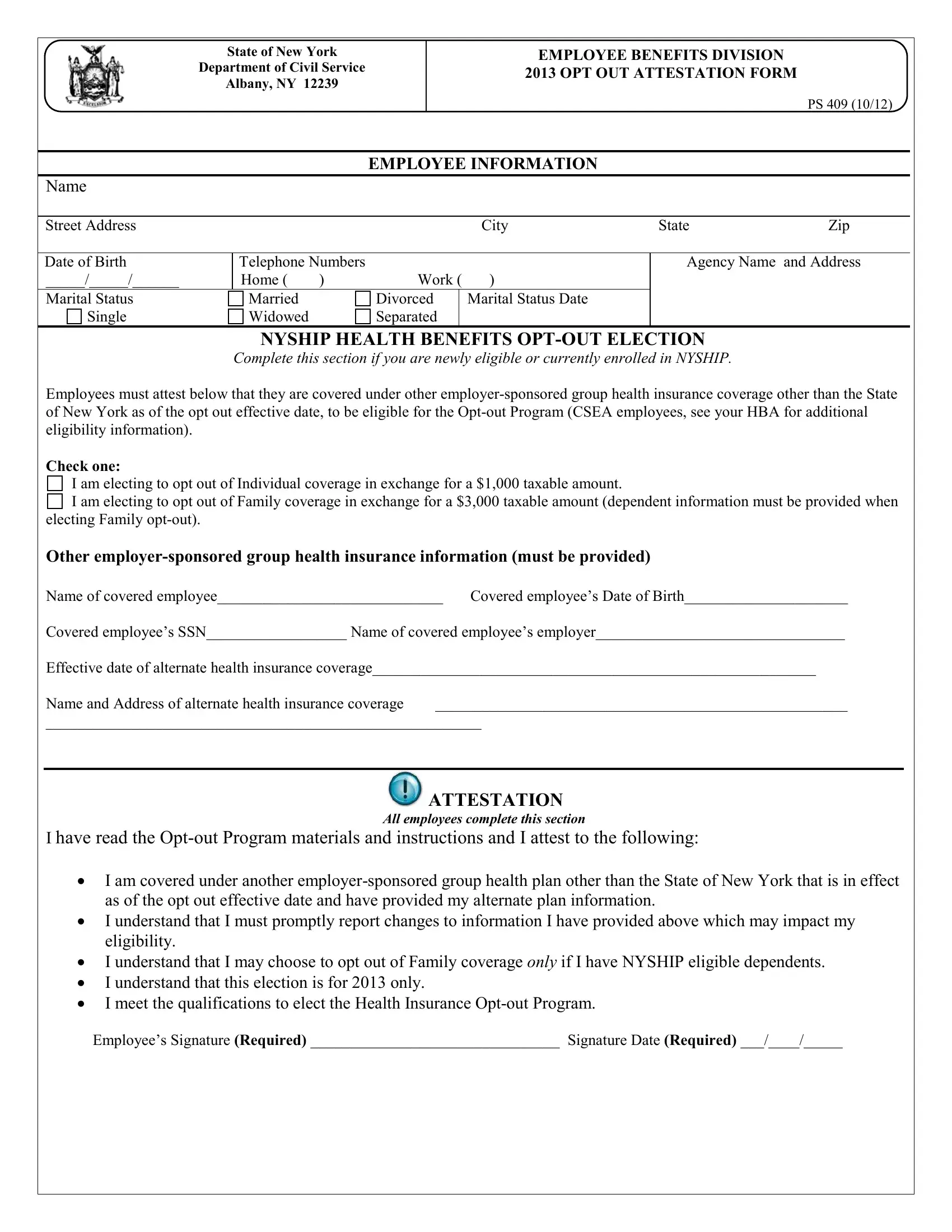
State of New York
Department of Civil Service
Albany, NY 12239
EMPLOYEE BENEFITS DIVISION 2013 OPT OUT ATTESTATION FORM
PS 409 (10/12)
EMPLOYEE INFORMATION
Name
Street Address |
City |
State |
Zip |
Date of Birth |
Telephone Numbers |
|
|
|
|
_____/_____/______ |
Home ( |
) |
Work ( |
) |
|
Marital Status |
Married |
|
Divorced |
|
Marital Status Date |
Single |
Widowed |
|
Separated |
|
|
|
|
|
|
|
|
Agency Name and Address
NYSHIP HEALTH BENEFITS
Complete this section if you are newly eligible or currently enrolled in NYSHIP.
Employees must attest below that they are covered under other
Check one:
I am electing to opt out of Individual coverage in exchange for a $1,000 taxable amount.
I am electing to opt out of Family coverage in exchange for a $3,000 taxable amount (dependent information must be provided when electing Family
Other
Name of covered employee_____________________________ Covered employee’s Date of Birth_____________________
Covered employee’s SSN__________________ Name of covered employee’s employer________________________________
Effective date of alternate health insurance coverage_________________________________________________________
Name and Address of alternate health insurance coverage _____________________________________________________
________________________________________________________
ATTESTATION
All employees complete this section
I have read the
•I am covered under another
•I understand that I must promptly report changes to information I have provided above which may impact my eligibility.
•I understand that I may choose to opt out of Family coverage only if I have NYSHIP eligible dependents.
•I understand that this election is for 2013 only.
•I meet the qualifications to elect the Health Insurance
Employee’s Signature (Required) ________________________________ Signature Date (Required) ___/____/_____
NYS Department of Civil Service |
Attestation Form |
|
Albany, NY 12239 |
Page 2 |
– PS 409 (10/12) |
Employees who can demonstrate and attest to having other
There are two circumstances when employees may elect to opt out of coverage; as newly eligible for the
INSTRUCTIONS:
Newly eligible employees: Employees may enroll in the
Current enrollees: Eligible enrollees may elect the
During
By signing the
The information you provide on this application is requested in accordance with Section 163 of New York State Civil Service Law for the principal purpose of enabling the Department of Civil Service to process your request concerning health insurance coverage. This information will be used in accordance with Section 96
(1)of the Personal Privacy Protection Law, particularly subdivisions (b), (e) and (f). Failure to provide the information requested may interfere with our ability to comply with your request. This information will be maintained by the Director of the Employee Benefits Division, NYS Department of Civil Service, Albany, NY 12239. For information concerning the Personal Protection Law, call (518)
or
This form is invalid if it is not signed and submitted along with a completed PS 404.