Navigating the intricacies of family and medical leave within the Newark Public Schools system can seem daunting at first glance. However, with the right information and understanding of the Newark Public Schools Lunch Application form, the process becomes clearer and more manageable. This comprehensive document not only outlines the procedures and requirements for applying for leave under the Family and Medical Leave Act (FMLA) and the New Jersey Family Leave Act (NJFLA) but also emphasizes the importance of communication between employees and their immediate supervisors during this process. It delineates eligibility criteria, such as the minimum months of service and hours worked, alongside the necessity of submitting a medical certificate. Moreover, the form underscores the district's commitment to support employees during their absence while ensuring minimal disruption to educational services. By providing detailed instructions on how to complete and submit the application, including necessary notices and medical certifications, the Newark Public Schools Lunch Application form serves as a critical resource for employees navigating the leave process, ultimately reflecting the district's broader mission to value and prioritize education even in the face of challenging circumstances.
| Question | Answer |
|---|---|
| Form Name | Newark Public Schools Lunch Application Form |
| Form Length | 8 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 2 min |
| Other names | newarkpublicschoolsfmlaforms, fmla new jersey application, how do i file for fmla in nj, emercency fmla in nj |
THE NEWARK PUBLIC SCHOOLS
Human Resource Services
Administrative Operation Services
Cami Anderson
State District Superintendent
Joseph Blundo
Interim Executive Director
2 Cedar Street, Rm811
Newark. New Jersey
Phone:
Fax:
Christopher D. Cerf Acting Commissioner of Education
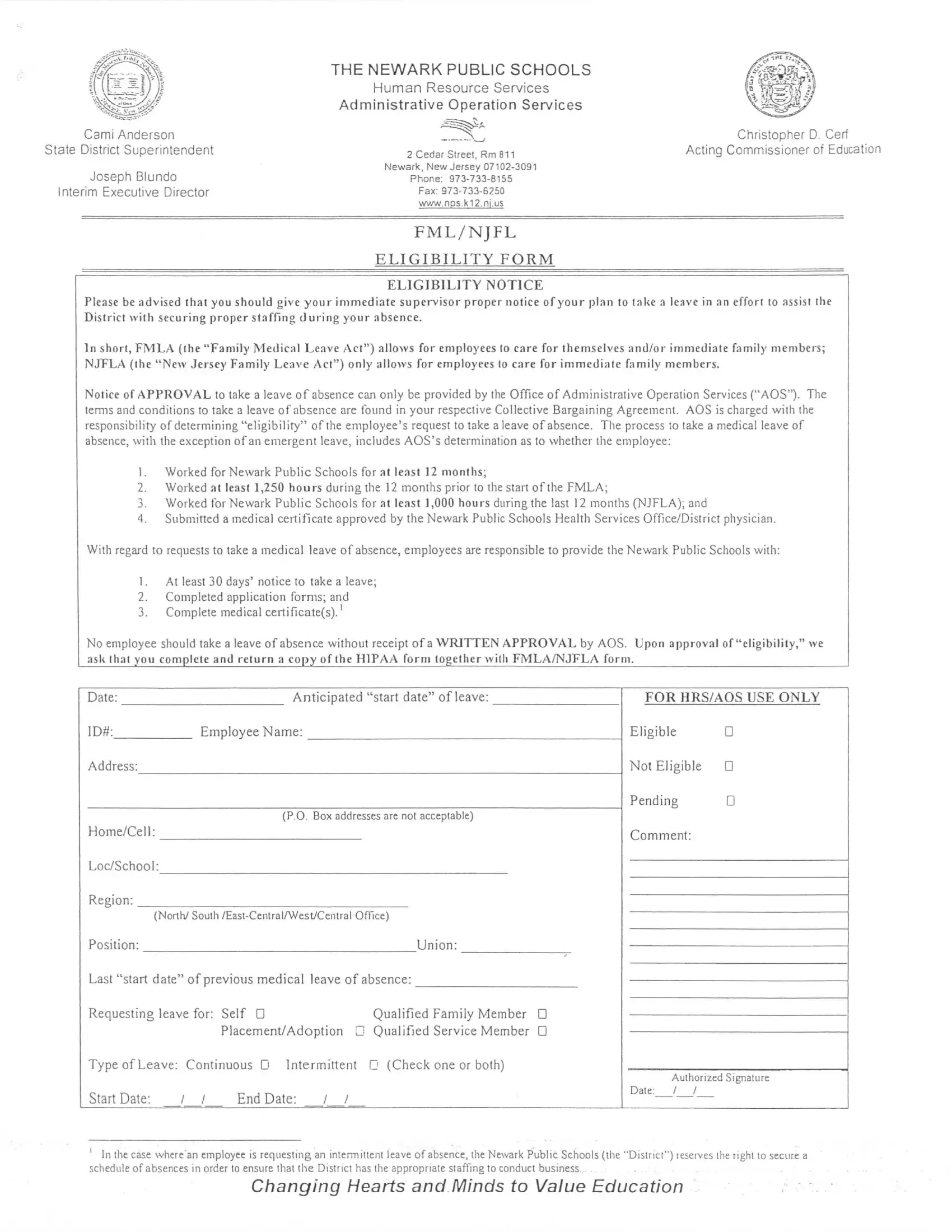
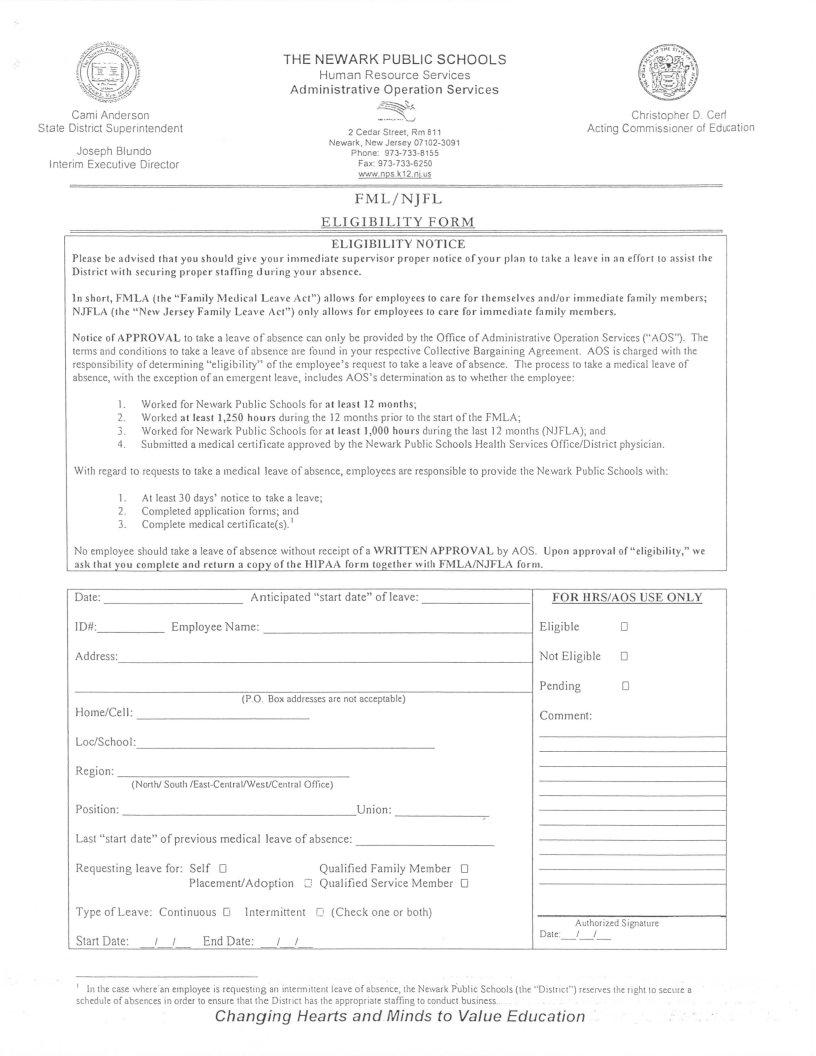
F M L / N J F L
E L I G I B I L I T Y F O R M
ELIGIBILITY NOTICE
Please be advised t h a t you s h o u l d give y o u r i m m e d i a t e supervisor proper notice of y o u r p l a n to t a k e a leave in an effort to assist the D i s t r i c t w i t h securing proper s t a f f i n g d u r i n g y o u r absence .
In short, FMLA ( t h e "Family Medical Leave Act") allows for employees to care for t h e m s e l v e s a n d / o r i m m e d i a t e f a m i l y members; NJTFLA ( t h e "New Jersey Family Leave Act") only allows for employees to care for i m m e d i a t e f a m i l y members .
Notice of APPROVAL to take a leave of absence can only be provided by the Office of Administrative Operation Services ("AOS"). The terms and conditions to take a leave of absence are found in your respective Collective Bargaining Agreement . AOS is charged with the responsibility of determining "eligibility" of the employee's request to take a leave of absence. The process to taJ<e a medical leave of absence, with the exception of an emergent leave, includes AOS's determination as to whether the employee:
1.Worked for Newark Public Schools for at least 12 m o n t h s ;
2.Worked at least 1,250 h o u r s d u r i n g the 12 months prior to the start of the FMLA;
3.Worked for Newark Public Schools for at least 1,000 hours during the last 12 months (NJFLA); and
4.Submitted a medical certificate approved by the Newark Public Schools Health Services Office/District physician.
With regard to requests to take a medical leave of absence, employees are responsible to provide the Newark Public Schools with:
1.At least 30 days' notice to take a leave;
2.Completed application forms; and
3.Complete medical certificate(s).1
No employee should take a leave of absence without receipt of a WRITTEN APPROVAL by AOS. Upon a p p r o v a l of "eligibility," we ask t h a t you c o m p l e t e and r e t u r n a copy of the H1PAA form t o g e t h e r w i t h FMLA/NJTXA form .
Date: |
Anticipated "start date" of leave: |
FOR HRS/AOS USE ONLY |
|
ID#: |
Employee Name: |
Eligible |
D |
Address: |
|
Not Eligible |
D |
|
|
Pending |
D |
|
(P.O. Box addresses are not acceptable) |
|
|
Home/Cell: |
|
Comment: |
|
Loc/School:
Region:
(North/
V
Type of Leave: Continuous D Intermittent n (Check one or both)
Start Date: / / End Date: / /
Authorized Signature
Date: / /
'In the case where'an employee is requesting an intermittent leave of absence, the Newark Public Schools (the "District") reserves the light to secure a schedule of absences in order to ensure that the District has the appropriate staffing to conduct business. ._.
Changing Hearts and Minds to Value Education
|
THE NEWARK PUBLIC SCHOOLS |
|
|
Human Resource Services |
|
|
Administrative OperationServices |
|
Cami Anderson |
|
Christopher D. Cerf |
State District Superintendent |
2 Cedar Street, Rm811 |
Acting Commissioner of Education |
|
|
|
Joseph Blundo |
Newark, New Jersey |
|
Phone: |
|
|
Interim Executive Director |
|
|
Fax: |
|
|
|
|
|
|
www.nps.K12.nj.us |
|
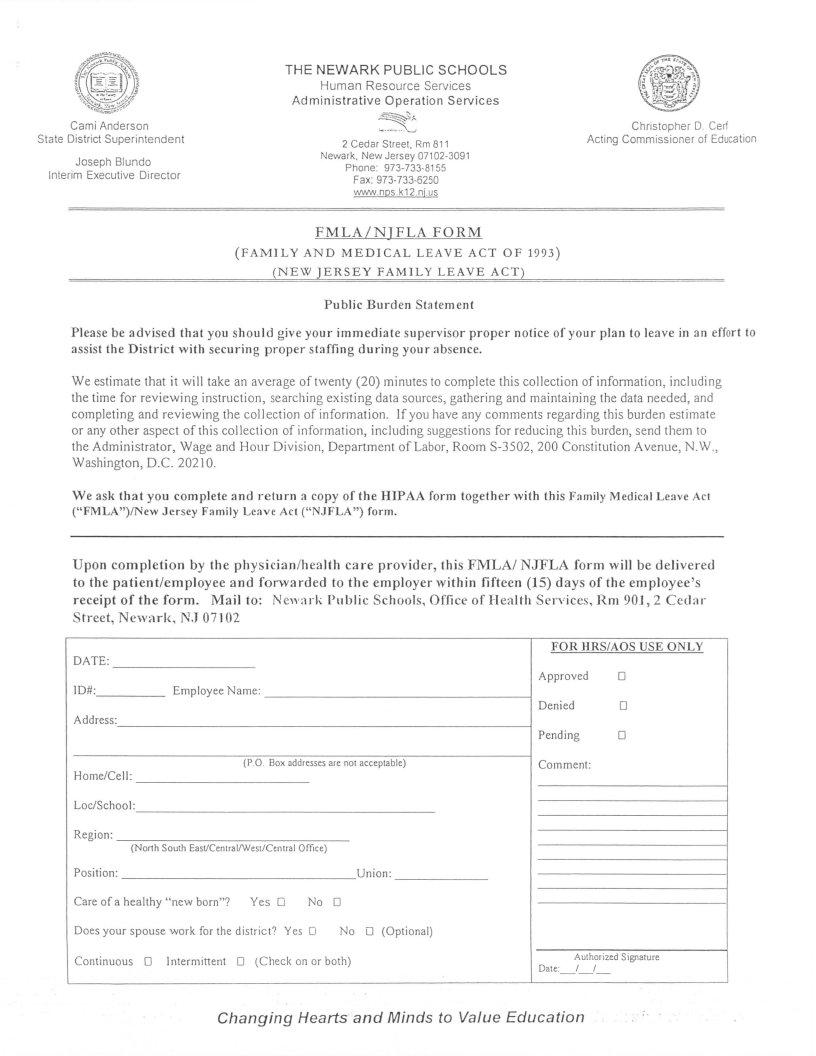
F M L A / N J F L A F O R M
(F A M I L Y A N D M E D I C A L L E A V E A C T O F 1993) ( N E W J E R S E Y F A M I L Y L E A V E ACT)
Public Burden Statement
Please be advised that you s h o u l d give your i m m e d i a t e supervisor proper notice of your plan to leave in an effort to assist the District with securing proper staffing d u r i n g your absence.
We estimate that it will take an average of twenty (20) minutes to complete this collection of information, including the time for reviewing instruction, searching existing data sources, gathering and maintaining the data needed, and completing and reviewing the collection of information. If you have any comments regarding this burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden, send them to the Administrator, Wage and Hour Division, Department of Labor, Room
We ask t h a t you complete and return a copy of the HIPAA form together with this Fnmily Medical Leave Act ("FMLA")/Ne\ Jersey Family Leave Act ("NJFLA") form.
Upon completion by the p h y s i c i a n / h e a l t h care provider, this FMLA/ NJFLA form will be delivered to the patient/employee and forwarded to the employer w i t h i n fifteen (15) days of the employee's receipt of the form. Mail to: N e w a r k P u b l i c Schools, Office of Health Services, Rm 90.1, 2 Cedar Street, Newark, N,J 07102
DATE:
1D#: |
Employee Name: |
Address:
(P.O. Box addresses are not acceptable)
Home/Cell:
Loc/School:
Region:
(North South East/Cenlral/West/Central Office)
Does your spouse work for the district? Yes D |
No D (Optional) |
Continuous D Intermittent D (Check on or both)
FOR HRS/AOS USE ONLY
Approved D
Denied D
Pending D
Comment:
Authorized Signature
Date: / /
Changing Hearts and Minds to Value Education
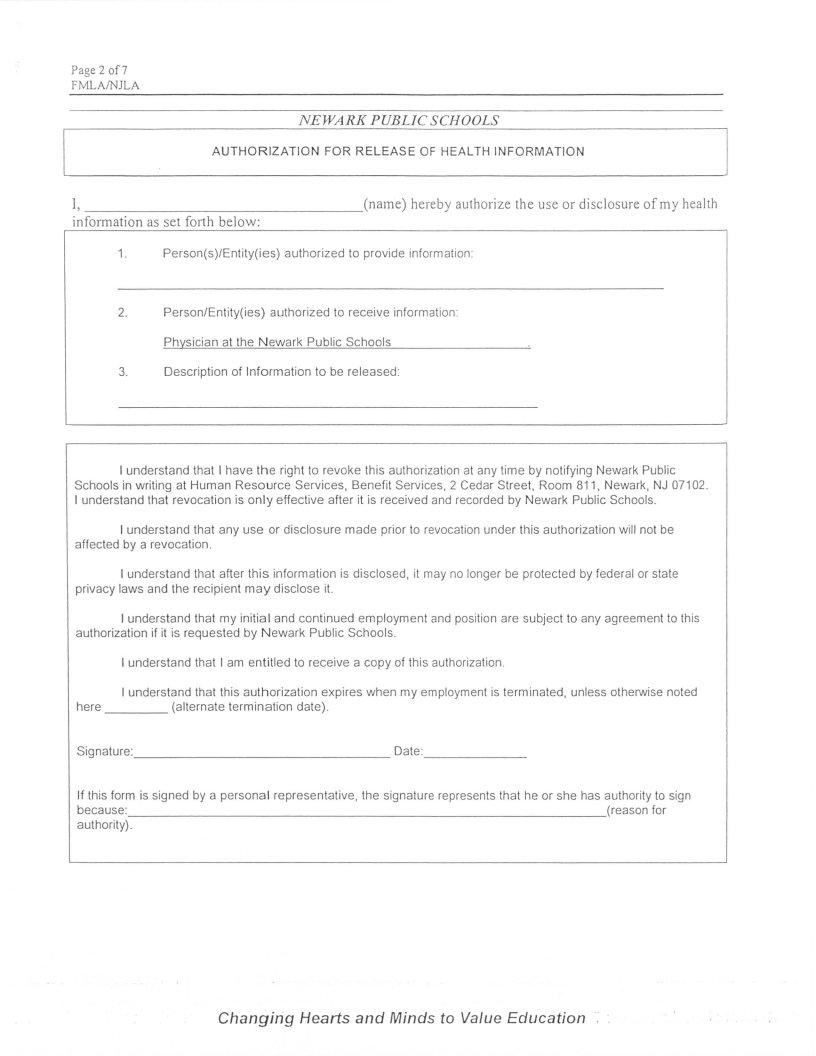
Page 2 of 7
FMLA/NJLA
NEWARK PUBLIC SCHOOLS
AUTHORIZATION FOR RELEASE OF HEALTH INFORMATION
I, |
(name) hereby authorize the use or disclosure of my health |
information as set forth below: |
|
1. Person(s)/Entity(ies) authorized to provide information:
2.Person/Entity(ies) authorized to receive information: Physician at the Newark Public Schools
3.Description of Information to be released:
I understand that I have the right to revoke this authorization at any time by notifying Newark Public Schools in writing at Human Resource Services, Benefit Services, 2 Cedar Street, Room 811, Newark, NJ 07102. I understand that revocation is only effective after it is received and recorded by Newark Public Schools.
I understand that any use or disclosure made prior to revocationunder this authorization will not be affected by a revocation.
I understand that after this information is disclosed, it may no longer be protected by federal or state privacy laws and the recipient may disclose it.
I understand that my initial and continued employment and position are subject to any agreement to this authorization if it is requested by Newark Public Schools.
I understand that I am entitled to receive a copy of thisauthorization.
I understand that this authorization expires when my employment is terminated, unless otherwise noted
here |
(alternate termination date). |
Signature: |
Date: |
If this form is signed by a personal representative, the signature represents that he or she has authority to sign
because:(reasonfor authority).
Changing Hearts and Minds to Value Education ".
Page 3 o f ?
FMLA/NJLA
THE FOLLOWING INFORMATION IS TO BE COMPLETED BY
YOUR HEALTH CARE PROVIDER
Print Name of Health Care Provider |
Signature of Health Care Provider |
Type of Practice |
Telephone Number |
Address |
Date |
1. Employee's Name |
2. Patient's Name (If different from employee) and age |
3.Relationshipto the family member/patient?
4.Does the patient's condition q u a l i f y under any of the categories described? "Yes" or "No"
If "Yes," please check the applicable category. (See "Definitions" below for description of "serious health condition" under the Family and Medical Leave Act ("FMLA")).
DHospital Care
DAbsence plus treatment
DPregnancy (EDC date: __/__/ (See page 6))
DChronic conditions requiring treatments
DPermanent/Long term conditions requiring supervision
DMultiple treatment for
DOther (please describe below)
5.Describe the medical facts which support the employee's certification. (Medical fact(s) include but is/are not limited to a Statement of Incapacity, diagnosis, prognosis, symptoms, abnormal laboratory results and physical findings, etc.) Attachments are acceptable.
Here and elsewhere on this form, the information sought relates only to the condition for which the employee is taking family medical leave.
Changing Hearts and Minds to Value Education
Page 4 of 7
FMLA/NJLA
6.a. State the time period of the absence for this period of incapacity (e.g., start and end date of incapacity) and the probable duration of the condition . (Please circle one.)
oStart date / / to 3 months
o6 months
o9 months
oother
b.What are the dates of the most recent visit(s) associated with the present episode of incapacity?
c.W i l l it be necessary for the employee to work only intermittently or to work on a less than a full
schedule as a result of the employee's condition (including for treatment described in item six (6) below)?
"Vf>c" n ™- "Mr," r D or "No" D
If "Yes," please give the probable duration of time needed for recovery.
d.If the condition is a chronic condition (condition #4) or pregnancy, state whether the patient is presently incapacitated and the likely duration and frequency of episodes of incapacity.
7.a. If additional visits will be required for the condition, provide an estimate of the probable number
of such visits (include date(s)).
If the patient will be absent from work or other daily activities because of visits/treatment on an intermittent or
b.If any of these treatments will be provided by another provider of health services (e.g., physical therapist), please state the nature of the treatments.
"Incapacity," for purposes of FMLA, is defined to mean inability to work, attend school or perform other regular daily activities due to the serious health condition, treatment thereof, or recovery there from.
Changing Hearts and Minds to Value Education
P a g e5 o f ?
FMLA/NJLA
c. If the employee is required to u n d e r g o a regimen of c o n t i n u i n g treatment under your supervision,please provide a general description of such regimen (e.g., prescription drugs, physical therapy requiring special equipment, etc.}.
8.a. If leave is required to care for a family member of the employee with a serious health condition, in what capacity will the employee be providing care to the family member?
TransportationD
PsychologicalD
Activities of daily l i v i n gD
Other (please describe below) D
b. If the employee will need care only intermittently or on a
Changing Hearts and Minds to Value Education
Page 6 of?
FMLA/NJLA
TO BE COMPLETED BY THE EMPLOYEE NEEDING FAMILY LEAVE TO CARE
FOR A FAMILY MEMBER
If the condition is pregnancy, please state the estimated dates of care and the care you w i l l provide during the period of care, including a schedule if leave is to be taken i n t e r m i t t e n t l y or if it will be necessary for you to work less than a full schedule.
I understand that per my request type, I am required to provide official documentation to the Newark Public Schools Health Services department at the time of application and upon my return when necessary. Without the required official documentation, the Human Resource Services department (HR) has the right to deny my request for leave or return at any time.
I understand that I must provide HR advanced written notice thirty (30) days prior to the start of my leave of absence. I further understand that my failure to timely return to work following the expiration of my authorized leave of absence may be construed as my voluntary resignation and/or subject me to disciplinary action.
Employee's Signature |
Dale |
Changing Hearts and Minds to Value Education
Page 7 of 7
FMLA/NJLA
DEFINITIONS:
A "Serious H e a l t h Condition" means an illness, i n j u r y impairment or physical/ mental condition that involves one of the following:
1 Hospital Care
I n p a t i e n t care (i.e.. an overnight stay) in hospital, hospice or residential medical care facility, including any period of incapacity or subsequent t r e a t m e n t in connection with or consequent to such i n p a t i e n t care.
2.Absence Plus Treatment
a)A period of incapacity of more t h a n t h r e e consecutive c a l e n d a r days (including any subsequent t r e a t m e n t or period of incapacity r e l a t i n g to the same condition) that also involves:
1)T r e a t m e n t two or m o r e times by a health care provider, nurse or physician's assistant under direct supervision of a health care provider or by a provider of health care services (g.g.. physical therapist under orders of or on referral by a health care provider;or
2)T r e a t m e n t by a health care provider on at least one occasion which results in a r e g i m e n of c o n t i n u i n g t r e a t m e n t ' 1 under the supervision of the health care provider.
3.Pregnancy
Any period ol incapacity due to p r e g n a n c y or p r e n a t a l care .
4. Chronic Conditions R e q u i r i n gTreatments
Ac h r o n i c c o n d i t i o n which:
a)Requires periodic visits for treatment by a health care provider, nurse or physician's assistant under direct supervision of a health care provider,
b)Continues over an e x t e n d e d period of t i m e ( i n c l u d i n g recurring episodes of s single underlying condition); and
c)May cause episodic rather than a continuing period of incapacity (e.g.. asthma, diabetes, epilepsy, etc.).
5.
Aperiod of i n c a p a c i t y which is p e r m a n e n t or long - term due to a condition for which treatment may not be effective . The employee or family member must be u n d e r the c o n t i n u e d s u p e r v i s i o n of, but need not be receiving active t r e a t m e n t by, a h e a l t h care provider . Examples include Alzheimer's, a severe stroke or the terminal stages of a disease.
6. M u l t i p l e Treatments
Any period of absence to receive m u l t i p l e t r e a t m e n t s ( i n c l u d i n g any period of recovery therefore) by a health care provider or by a provider of health care services under orders of or on referral by a health care provider, either for restorative surgery after an accident or other injury or for a condition that would likely result in a period of incapacity of more t h a n three consecutive c a l e n d a r days in t h e absence of m e d i c a l i n t e r v e n t i o n or t r e a t m e n t , such as cancer (chemotherapy, radiation, etc.), severe arthritis (physical therapy), and kidney disease (dialysis) .
This optional form may be used by employees to satisfy a mandatory requirement to furnish a medical certification (when requested) from a health care provider, including second or third opinions and recertification (29 CFR 825.306).
Note: Persons are not required to respond to this collection of information unless it displays a currently valid OMB control number .
3 A regimen of continuing treatment includes, for example, a course of prescription medication (e.g., an antibiotic) or therapy requiring special equipment to resolve or alleviate the health condition. A regimen of treatment does not include the taking of
Changing Hearts and Minds to Value Education