
Should you would like to fill out doj nh charitable, there's no need to download and install any sort of software - just use our PDF tool. Our editor is consistently developing to present the very best user experience attainable, and that is because of our commitment to constant development and listening closely to customer feedback. If you are looking to begin, here's what it will take:
Step 1: Click the "Get Form" button at the top of this webpage to access our PDF editor.
Step 2: Using this online PDF file editor, you are able to do more than merely fill out blanks. Try each of the features and make your documents appear sublime with customized text added in, or optimize the file's original input to perfection - all that comes along with an ability to insert your own images and sign it off.
In an effort to complete this document, be sure you enter the required details in each field:
1. While filling out the doj nh charitable, be certain to include all essential blanks in the relevant part. This will help facilitate the process, which allows your information to be processed efficiently and correctly.
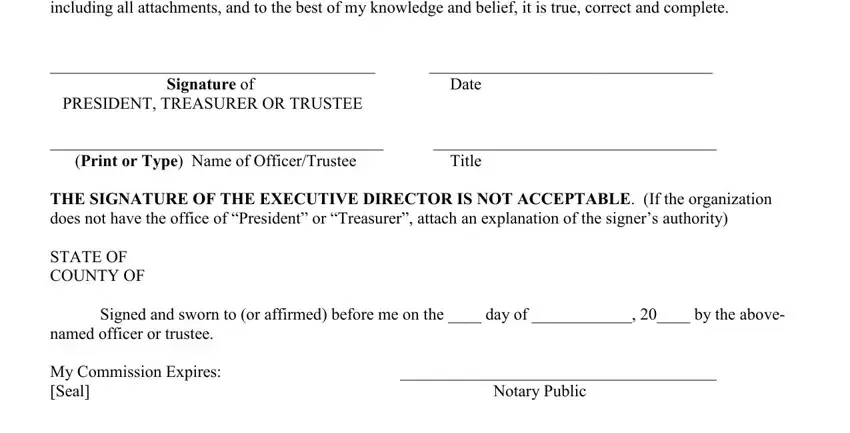
2. Once your current task is complete, take the next step – fill out all of these fields - ANNUAL FILING FEE Make check, Signed and sworn to or affirmed, Notary Public, Title, and Date with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
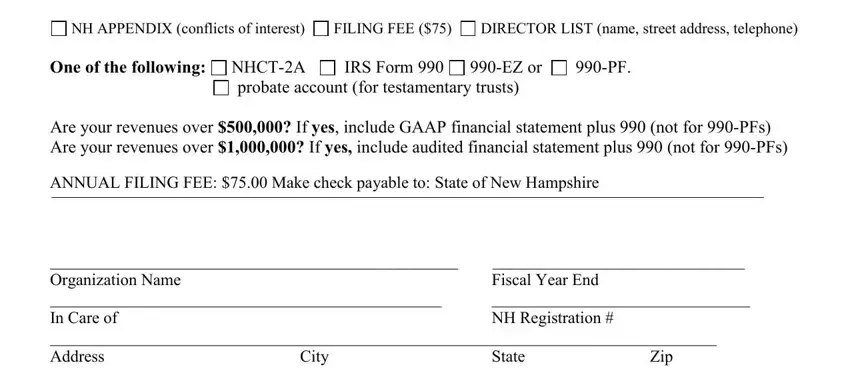
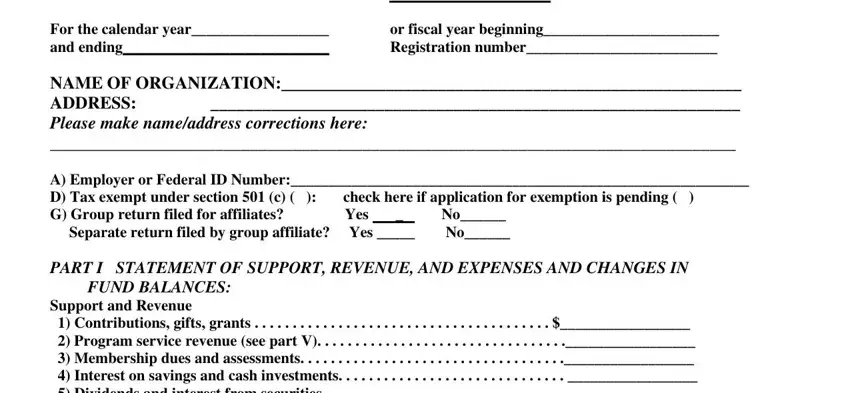
3. This next portion is mostly about ANNUAL REPORT, or fiscal year beginning, and For the calendar year and ending - fill out all of these blank fields.
Always be really attentive when filling in or fiscal year beginning and ANNUAL REPORT, as this is the section in which most users make mistakes.
4. Filling in For the calendar year and ending, a Gross revenue, Fund Balances Lines Through Must, and ATTACH EXPLANATION is essential in the fourth section - ensure to spend some time and take a close look at every blank!
5. As you draw near to the conclusion of this file, you will find several extra requirements that must be satisfied. Specifically, Organization Name PART II should be done.
Step 3: Revise all the details you have typed into the form fields and press the "Done" button. Grab your doj nh charitable the instant you join for a free trial. Conveniently access the form inside your personal account page, together with any edits and adjustments being conveniently synced! Here at FormsPal.com, we do everything we can to guarantee that all of your details are stored private.