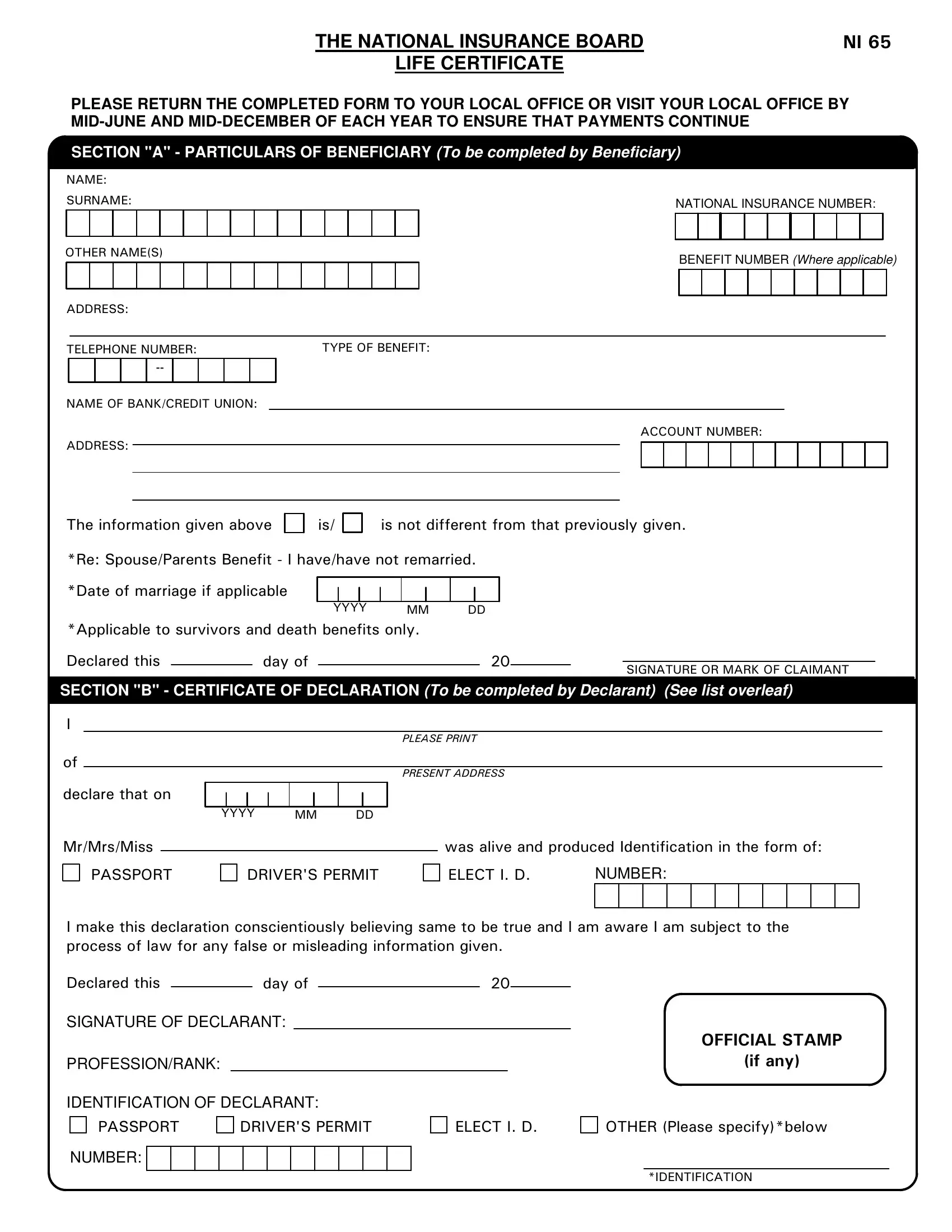
Ensuring the continuous provision of benefits for its recipients, the National Insurance Board's NI 65 Life Certificate plays a crucial role. To be submitted biannually by mid-June and mid-December, this document seeks to affirm the ongoing life status of beneficiaries receiving various forms of assistance, such as retirement, invalidity and disablement pensions, survivors' benefits, and employment injury death benefits. Carefully divided into two main sections, the form calls for detailed beneficiary particulars—including name, address, national insurance and benefit numbers, and banking details—in Section "A". Meanwhile, Section "B" obligates a trustworthy declarant to certify the beneficiary's status, underpinned by solid identification markers like passports and driver's permits. Recognizing the form's importance in warding off any disruptions in payment, it prescribes a straightforward yet comprehensive verification mechanism for residents both within and outside Trinidad and Tobago, involving respected community members and officials. This structured approach underscores the commitment to maintain the integrity of the benefits system, while also addressing the practicalities of confirming beneficiaries' circumstances and ensuring rightful disbursement of aid.
| Question | Answer |
|---|---|
| Form Name | Ni 65 Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | ni 65 forms trinidad, nibtt, ni82 form, ni 82 |
THE NATIONAL INSURANCE BOARD |
NI 65 |
LIFE CERTIFICATE |
|
PLEASE RETURN THE COMPLETED FORM TO YOUR LOCAL OFFICE OR VISIT YOUR LOCAL OFFICE BY
SECTION "A" - PARTICULARS OF BENEFICIARY (To be completed by Beneficiary)
NAME:
SURNAME: |
|
NATIONAL INSURANCE NUMBER: |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OTHER NAME(S)
ADDRESS:
BENEFIT NUMBER (Where applicable)
TELEPHONE NUMBER: |
TYPE OF BENEFIT: |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAME OF BANK/CREDIT UNION: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
ACCOUNT NUMBER: |
|||||||||||
ADDRESS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
The information given above |
is/ |
is not different from that previously given. |
|||||||||||||
*Re: Spouse/Parents Benefit - I have/have not remarried. |
|
|
|
||||||||||||
*Date of marriage if applicable |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
YYYY |
|
MM |
DD |
|
|
|
||||||
*Applicable to survivors and death benefits only. |
|
|
|
|
|
|
|
||||||||
Declared this |
|
day of |
|
|
|
|
|
|
|
20 |
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE OR MARK OF CLAIMANT |
||||
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SECTION "B" - CERTIFICATE OF DECLARATION (To be completed by Declarant) (See list overleaf)
I
PLEASE PRINT
of
PRESENT ADDRESS
declare that on
Mr/Mrs/Miss
PASSPORT
YYYY MM DD
DRIVER'S PERMIT
was alive and produced Identification in the form of:
ELECT I. D. |
NUMBER: |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
I make this declaration conscientiously believing same to be true and I am aware I am subject to the process of law for any false or misleading information given.
Declared this |
|
day of |
|
20 |
|
|
SIGNATURE OF DECLARANT:
PROFESSION/RANK:
IDENTIFICATION OF DECLARANT:
PASSPORT |
DRIVER'S PERMIT |
ELECT I. D. |
NUMBER:
OFFICIAL STAMP
(if any)
OTHER (Please specify)*below
*IDENTIFICATION
2/NI 65
INSTRUCTIONS FOR USE OF LIFE CERTIFICATE
(The purpose of the Life Certificate is to establish that the
beneficiary is alive on the date of this Declaration)
1.All Recipients of National Insurance Retirement, Invalidity and Disablement Pensions, Survivors Benefits and Employment Injury Death Benefits must complete this LifeCertificate every six months.
2.The Declaration may be signed by:
(a)(For a resident of Trinidad and Tobago)
any Magistrate, Justice of the Peace, Clergyman, Warden, Councillor/Assemblyman, Bank Manager, Medical Practitioner,
(b)(For a
a member of the Trinidad and Tobago Mission in the Country in which the Beneficiary is a resident OR an
3.Identification produced by the beneficiary should be a valid form of one of the following: Passport, Driver's Permit or Electoral Identification Card.
4.You are required to submit a BANK ACCOUNT NUMBER as provided for on this Form.