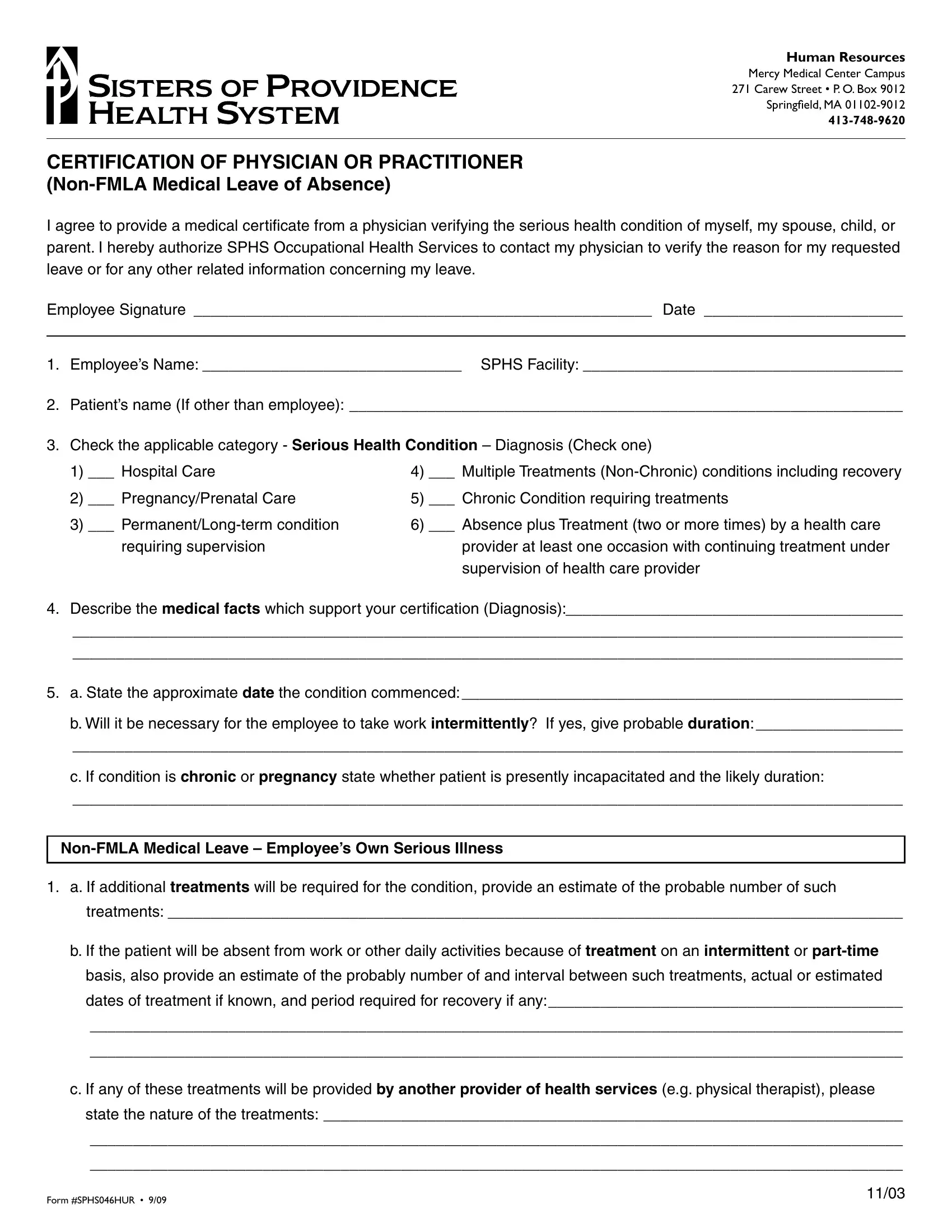
HUMAN RESOURCES
Mercy Medical Center Campus 271CarewStreet•P.O.Box9012 Springield,MA01102-9012
413-748-9620
CERTIFICATION OF PHYSICIAN OR PRACTITIONER
(Non-FMLA Medical Leave of Absence)
I agree to provide a medical certificate from a physician verifying the serious health condition of myself, my spouse, child, or parent. I hereby authorize SPHS Occupational Health Services to contact my physician to verify the reason for my requested leave or for any other related information concerning my leave.
Employee Signature _____________________________________________________ Date _______________________
1. Employee’s Name: ______________________________ SPHS Facility: _____________________________________
2.Patient’s name (If other than employee): ________________________________________________________________
3.Check the applicable category - Serious Health Condition – Diagnosis (Check one)
1) |
___ Hospital Care |
4) |
___ Multiple Treatments (Non-Chronic) conditions including recovery |
2) |
___ Pregnancy/Prenatal Care |
5) |
___ Chronic Condition requiring treatments |
3) |
___ Permanent/Long-term condition |
6) |
___ Absence plus Treatment (two or more times) by a health care |
|
requiring supervision |
|
provider at least one occasion with continuing treatment under |
|
|
|
supervision of health care provider |
4.Describe the medical facts which support your certification (Diagnosis):_______________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
5.a. State the approximate date the condition commenced: ___________________________________________________
b.Will it be necessary for the employee to take work intermittently? If yes, give probable duration: _________________
________________________________________________________________________________________________
c.If condition is chronic or pregnancy state whether patient is presently incapacitated and the likely duration:
________________________________________________________________________________________________
Non-FMLA Medical Leave – Employee’s Own Serious Illness
1.a. If additional treatments will be required for the condition, provide an estimate of the probable number of such treatments: _____________________________________________________________________________________
b.If the patient will be absent from work or other daily activities because of treatment on an intermittent or part-time basis, also provide an estimate of the probably number of and interval between such treatments, actual or estimated dates of treatment if known, and period required for recovery if any:_________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
c.If any of these treatments will be provided by another provider of health services (e.g. physical therapist), please state the nature of the treatments: ___________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
Form#SPHS046HUR • 9/09 |
11/03 |
|

d.If a regimen of continuing treatment by the patient is required under your supervision, provide a general description of such regimen (e.g., prescription drugs, physical therapy requiring special equipment): ________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
2.a. If medical leave is required for the employee’s absence from work because of the employee’s own condition (including absences due to pregnancy or a chronic condition), is the employee unable to perform work of any kind? explain: ________________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
b.If able to perform some work, is the employee unable to perform any one or more of the essential functions of the employee’s job (the employee or the employer should supply you with information about the essential job functions)? If yes, please list the essential functions of the employee is unable to perform:_________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
c.If neither a nor b applies, is it necessary for the employee to be absent from work for treatment? Explain: _________
______________________________________________________________________________________________
______________________________________________________________________________________________
Non-FMLA Medical Leave – To Care for Seriously ILL Family Member:
1.a. If leave is required to care for a family member of the employee with a serious health condition, does the patient require assistance for basic medical or personal needs or safety or for transportation? Explain: __________________
______________________________________________________________________________________________
______________________________________________________________________________________________
b.If no, would the employee’s presence to provide psychological comfort be beneficial to the patient or assist in the patient’s recovery? Explain: ________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
c.If the patient will need care only intermittently or on a part-time basis, please indicate the probable duration of
this need: ______________________________________________________________________________________
______________________________________________________________________________________________
______________________________________________________________________________________________
2.State the care you will provide and an estimate of the period during which care will be provided, including a schedule if leave is to be taken intermittently or if it will be necessary for you to work less than a full schedule: __________________
________________________________________________________________________________________________
________________________________________________________________________________________________
________________________________________________________________________________________________
______________________________________________________________ |
__________________________________ |
Signature of Physician or Practitioner |
Type of Practice: |
______________________________________________________________ |
__________________________________ |
Address |
Telephone Number |
______________________________________________________________ |
__________________________________ |
|
Date |