Are you new to North Carolina and curious about the tax forms that you need to file? Figuring out each state's unique form requirements can be tricky, but don't worry—we've got you covered! In this blog post, we’ll go over everything you need to know about the North Carolina Form 90. We'll explain what it is, when it needs to be filed, and how doing so can help your finances in the long run. So keep reading if you want to learn more about how filing a North Carolina Form 90 could benefit your future financial situation.
| Question | Answer |
|---|---|
| Form Name | North Carolina Form 90 |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | form90 pd 107 fillable form |
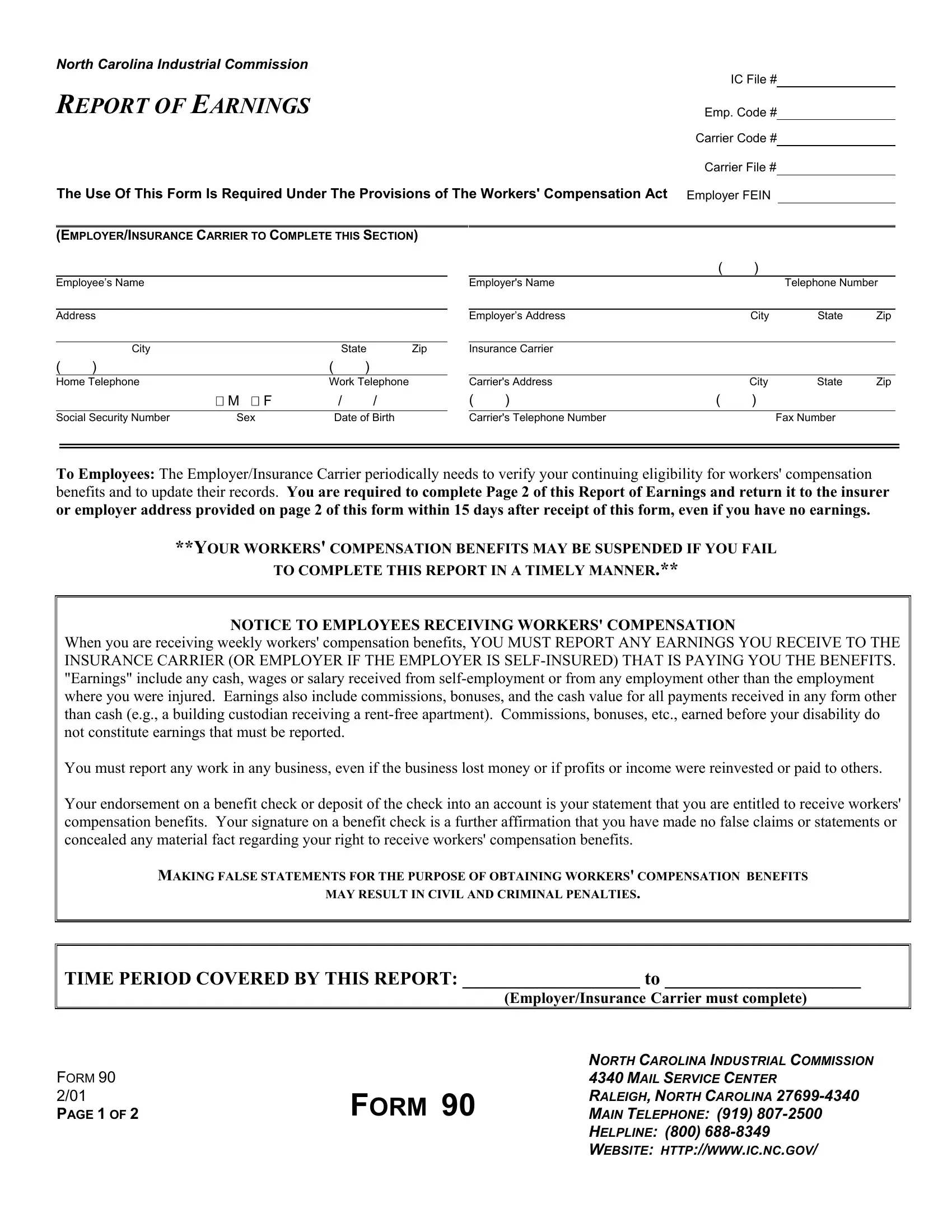
NORTH CAROLINA INDUSTRIAL COMMISSION
IC File #
REPORT OF EARNINGS
Emp. Code #
Carrier Code #
Carrier File #
The Use Of This Form Is Required Under The Provisions of The Workers' Compensation Act Employer FEIN
(EMPLOYER/INSURANCE CARRIER TO COMPLETE THIS SECTION)
Employee’s Name
Address
|
City |
|
|
State |
Zip |
( |
) |
|
( |
) |
|
Home Telephone |
|
Work Telephone |
|||
|
|
M F |
|
/ |
/ |
|
|
|
|
||
Social Security Number |
Sex |
|
Date of Birth |
||
|
|
( |
) |
|
|
Employer's Name |
|
|
Telephone Number |
||
|
|
|
|
|
|
Employer’s Address |
|
City |
State |
Zip |
|
|
|
|
|
|
|
Insurance Carrier |
|
|
|
|
|
|
|
|
|
|
|
Carrier's Address |
|
City |
State |
Zip |
|
( |
) |
( |
) |
|
|
|
|
|
|
|
|
Carrier's Telephone Number |
|
|
Fax Number |
|
|
To Employees: The Employer/Insurance Carrier periodically needs to verify your continuing eligibility for workers' compensation benefits and to update their records. You are required to complete Page 2 of this Report of Earnings and return it to the insurer or employer address provided on page 2 of this form within 15 days after receipt of this form, even if you have no earnings.
**YOUR WORKERS' COMPENSATION BENEFITS MAY BE SUSPENDED IF YOU FAIL
TO COMPLETE THIS REPORT IN A TIMELY MANNER.**
NOTICE TO EMPLOYEES RECEIVING WORKERS' COMPENSATION
When you are receiving weekly workers' compensation benefits, YOU MUST REPORT ANY EARNINGS YOU RECEIVE TO THE INSURANCE CARRIER (OR EMPLOYER IF THE EMPLOYER IS
You must report any work in any business, even if the business lost money or if profits or income were reinvested or paid to others.
Your endorsement on a benefit check or deposit of the check into an account is your statement that you are entitled to receive workers' compensation benefits. Your signature on a benefit check is a further affirmation that you have made no false claims or statements or concealed any material fact regarding your right to receive workers' compensation benefits.
MAKING FALSE STATEMENTS FOR THE PURPOSE OF OBTAINING WORKERS' COMPENSATION BENEFITS
MAY RESULT IN CIVIL AND CRIMINAL PENALTIES.
TIME PERIOD COVERED BY THIS REPORT: ___________________ to _____________________
(Employer/Insurance Carrier must complete)
FORM 90 2/01
PAGE 1 OF 2
FORM 90
NORTH CAROLINA INDUSTRIAL COMMISSION
4340 MAIL SERVICE CENTER
RALEIGH, NORTH CAROLINA
MAIN TELEPHONE: (919)
HELPLINE: (800)
WEBSITE: HTTP://WWW.IC.NC.GOV/
EMPLOYEE: COMPLETE SECTION BELOW
(1) Did you receive earnings from work during the time period
indicated on Page 1? |
YES |
NO |
(2) Did you work for a business or any person during that time
period? |
YES |
NO |
(3)If you answered NO to both questions 1 and 2, sign and return the form to the insurance carrier or to the individual identified by the insurance carrier or employer listed below.
(4)If you answer YES to either question, complete item 5 below, sign and return the form to the insurance carrier or to the individual identified by the insurance carrier or employer listed below. For the purposes of this statement, “Gross Earnings” include all
(5)1st Employer or Business Name (include
Location:
Dates worked:
Gross Earnings:
Next Employer or Business Name (include
Location:
Dates worked:
Gross Earnings:
Attach additional page(s) if necessary.
Employee Signature: |
|
Date: |
|
. |
(Required)
NOTICE TO EMPLOYEE:
1.Failure to report earnings as defined herein may subject you to criminal prosecution and civil liability including the suspension or forfeiture of your benefits. This form must be signed and returned to the insurance carrier listed below even if you have no earnings.
2.If the Commission suspends benefits for failure to complete and return a Form 90 Report of Earnings, the
3.If benefits are not immediately reinstated, the employee should submit a written request for an Order from the Executive Secretary instructing the employer or insurance carrier to reinstate benefits. An application for reinstatement of benefits should be addressed to North Carolina Industrial Commission, Office of the Executive Secretary, 4333 Mail Service Center, Raleigh, NC
Insurance carrier or Employer must list the name and address below of the person to whom this form must be returned and mail this form to the employee by certified mail return receipt requested, and include a
Name: |
|
|
|
. |
||
Address: |
|
|
|
. |
||
|
|
City |
State |
Zip |
||
|
|
|
|
|
|
|
NOTICE TO INSURER OR EMPLOYER:
Any person who willfully makes a false statement or representation of a material fact for the purpose of denying or assisting another in denying any benefit or payment under the Workers’ Compensation Act shall be guilty of a Class 1 misdemeanor if the amount at issue is less than $1000. Violation is a Class H felony if the amount at issue exceeds $1000. Any person who threatens an employee with criminal prosecution under the provisions of the Act for the purpose of coercing or attempting to coerce an employee into agreeing to compensation under the Act shall be guilty of a Class H felony.
FORM 90 2/01
PAGE 2 OF 2
FORM 90
NORTH CAROLINA INDUSTRIAL COMMISSION
4340 MAIL SERVICE CENTER
RALEIGH, NORTH CAROLINA
MAIN TELEPHONE: (919)
HELPLINE: (800)
WEBSITE: HTTP://WWW.IC.NC.GOV/