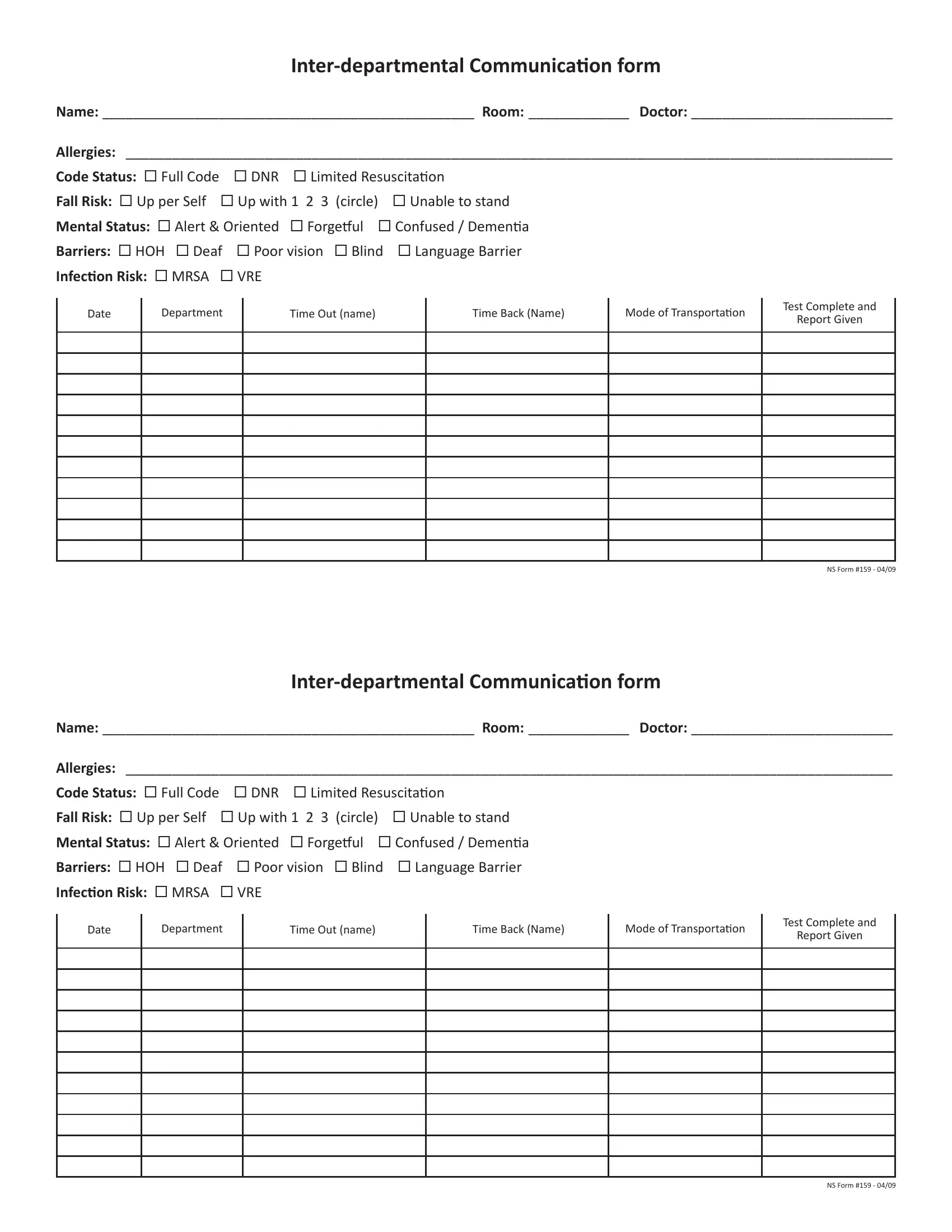
In the landscape of healthcare communication, the Inter-departmental Communication Form, known as NS Form #159, serves as a crucial conduit for patient information across different departments. This form covers a broad spectrum of patient details that are essential for providing comprehensive care, making it an indispensable tool for healthcare providers. These details include the patient’s name, room number, attending doctor, a list of allergies, code status (such as Full Code, DNR, or Limited Resuscitation), fall risk assessment, mental status, barriers to communication (such as Hard of Hearing, Deaf, Poor Vision, Blind, or Language Barrier), infection risks like MRSA or VRE, and even the logistics related to the patient’s movement between departments. Detailed sections about the test, department involved, mode of transportation, and timestamps for departure and return, further ensure that the communication loop is closed and nothing is left to chance. Grounded in the principle of patient safety and efficiency, NS Form #159 epitomizes how structured communication can enhance the coordination of care and facilitate a seamless healthcare experience.
| Question | Answer |
|---|---|
| Form Name | Ns Form 159 |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | VRE, DNR, departmental, Forgetful |

Name: ________________________________________________ Room: _____________ Doctor: __________________________
Allergies: ___________________________________________________________________________________________________
Code Status: Full Code |
DNR Limited Resuscitaion |
|
Fall Risk: Up per Self |
Up with 1 2 3 (circle) |
Unable to stand |
Mental Status: Alert & Oriented Forgeful Confused / Demenia |
||
Barriers: HOH Deaf Poor vision Blind |
Language Barrier |
|
Infecion Risk: MRSA |
VRE |
|
Date
Department
Time Out (name)
Time Back (Name)
Mode of Transportaion
Test Complete and
Report Given
NS Form #159 - 04/09
Name: ________________________________________________ Room: _____________ Doctor: __________________________
Allergies: ___________________________________________________________________________________________________
Code Status: Full Code |
DNR Limited Resuscitaion |
|
Fall Risk: Up per Self |
Up with 1 2 3 (circle) |
Unable to stand |
Mental Status: Alert & Oriented Forgeful Confused / Demenia |
||
Barriers: HOH Deaf Poor vision Blind |
Language Barrier |
|
Infecion Risk: MRSA |
VRE |
|
Date
Department
Time Out (name)
Time Back (Name)
Mode of Transportaion
Test Complete and
Report Given
NS Form #159 - 04/09