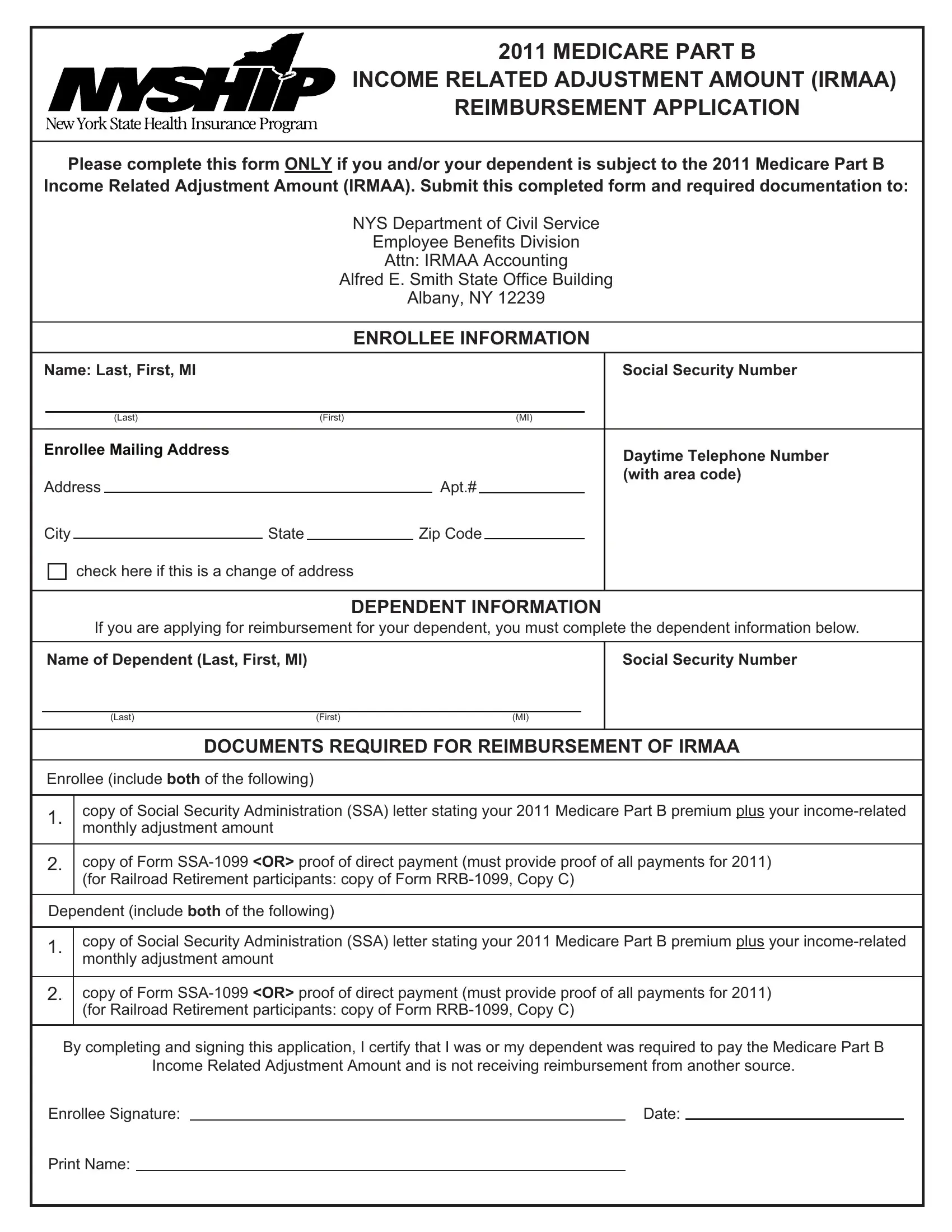
The New York State Health Insurance Program (NYSHIP) provides a vital service for its enrollees, one aspect of which includes the potential reimbursement for the Medicare Part B Income Related Adjustment Amount (IRMAA). The process to apply for this reimbursement is predominantly articulated through the specific form designed for the year 2011. This form is a crucial document for those who were subject to the IRMAA, allowing them, as well as their dependents, to claim a refund for the additional premiums paid. To navigate this process efficiently, the form mandates the submission of several pieces of information and documentation, including personal details, social security numbers, and a copy of the SSA letter that verifies the premium and adjustment amount. Furthermore, it insists on documentation proving the payment of these adjusted premiums, amidst other requirements, aiming to validate the eligibility for reimbursement. The form serves not only as an application but also as a formal certification by the enrollee, asserting their entitlement to reimbursement, precluding those already compensated from other sources. The outlined procedure underscores the significance of timely submission and the procedural steps necessary for the Employee Benefits Division to process these claims, spotlighting the broader commitment of NYSHIP to safeguarding the financial interests of its members against unforeseen adjustments in their Medicare Part B premiums.
| Question | Answer |
|---|---|
| Form Name | Nyship Form |
| Form Length | 2 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 30 sec |
| Other names | irmaa 2020 reimbursement application, irmaa 2020 form, nyc irmaa 2020 form, nyc irmaa reimbursement 2020 |
2011 MEDICARE PART B
INCOME RELATED ADJUSTMENT AMOUNT (IRMAA)
REIMBURSEMENT APPLICATION
Please complete this form ONLY if you and/or your dependent is subject to the 2011 Medicare Part B
Income Related Adjustment Amount (IRMAA). Submit this completed form and required documentation to:
NYS Department of Civil Service
Employee Benefits Division
Attn: IRMAA Accounting
Alfred E. Smith State Office Building
Albany, NY 12239
|
|
|
|
|
|
ENROLLEE INFORMATION |
|||||
|
|
|
|
|
|
|
|
|
|
|
|
Name: Last, First, MI |
|
|
|
|
|
|
|
Social Security Number |
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Last) |
|
(First) |
|
|
|
|
(MI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
Enrollee Mailing Address |
|
|
|
|
|
|
|
Daytime Telephone Number |
|||
|
|
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
|
Apt.# |
|
|
(with area code) |
||
|
|
|
|
|
|
|
|
||||
City |
|
State |
|
|
Zip Code |
|
|
||||
check here if this is a change of address
DEPENDENT INFORMATION
If you are applying for reimbursement for your dependent, you must complete the dependent information below.
Name of Dependent (Last, First, MI)
(Last) |
(First) |
(MI) |
Social Security Number
DOCUMENTS REQUIRED FOR REIMBURSEMENT OF IRMAA
Enrollee (include both of the following)
1.copy of Social Security Administration (SSA) letter stating your 2011 Medicare Part B premium plus your
2.copy of Form
Dependent (include both of the following)
1.copy of Social Security Administration (SSA) letter stating your 2011 Medicare Part B premium plus your
2.copy of Form
By completing and signing this application, I certify that I was or my dependent was required to pay the Medicare Part B
Income Related Adjustment Amount and is not receiving reimbursement from another source.
Enrollee Signature: |
|
Date: |
Print Name:
IRMAA reimbursement for both the enrollee and dependent will be issued to the enrollee ONLY. In order for the Employee Benefits Division to speak with the dependent regarding the application for the Income Related Medicare Adjustment Amount (IRMAA), we must have a HIPAA Release Form
If you need a replacement copy of your 2011 IRMAA notice, which was mailed to you in late 2010, contact your local Social Security office. The location of your local office can be found in your local telephone book or at: www.socialsecurity.gov/onlineservices. This website can also be accessed to request a replacement copy of the form
You are encouraged to submit your request for NYSHIP reimbursement no later than May 31, 2012. Refunds will be sent as a separate check to your address of record. The refund process will take a minimum of
Medicare Part B Premium Reimbursement From Another Source
Complete the following if you and/or your covered dependent receives full or partial Medicare Part B premium reimbursement from another source, such as your spouse’s former employer:
Enrollee/Dependent Name |
|
Reimbursement Source |
|
Amount or % (per month) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Personal Privacy Protection Law Notification: The information you provide on this form is requested for the principal purpose of authorizing the use and/or disclosure of protected health information pursuant to 45 CFR 164.508. Failure to provide the information may interfere with our ability to use or disclose protected health information necessary to administer NYSHIP and NYPERL. The information will be maintained by the Director of the Employee Benefits Division, Department of Civil Service, Albany, NY 12239. The information will be used in accordance with Public Officers Law section 96(1), also known as the Personal Privacy Protection Law. For information on the Personal Privacy Protection Law, call (518)
IRMAA 2011 APPL