In today's healthcare landscape, ensuring that the right support is available for those needing occupational therapy is crucial. The Occupational Therapy Referral Checklist form plays an essential role in streamlining this process, assisting occupational therapists and other professionals in determining a patient's need for occupational therapy services. Designed with the input of therapists to include language that is accessible and focused on the core aspects of traditional occupational therapy, this form is a foundational tool intended not to replace detailed assessments but to guide the initial stages of intervention. Organized around the significant themes from the Model of Human Occupation—volition, habituation, performance, and environment—it allows therapists to make a well-informed judgment on a client's need for therapy. Key areas such as confidence, self-care, productivity, leisure, interpersonal skills, cognitive and physical abilities, and environmental factors are evaluated, providing a clear picture of a client’s functioning across a broad spectrum. Completing the checklist involves a discussion with someone already working with the client, ensuring a comprehensive view of the client's needs and circumstances. By offering a structured way to screen and prioritize referrals, this checklist ensures the most efficient use of limited occupational therapy resources, focusing on areas where intervention can have the most significant impact.
| Question | Answer |
|---|---|
| Form Name | Occupational Therapy Referral Checklist Form |
| Form Length | 2 pages |
| Fillable? | Yes |
| Fillable fields | 47 |
| Avg. time to fill out | 9 min 54 sec |
| Other names | Occupational Therapy Referral Priority Checklist Form, Physical Therapy Referral Checklist Form |
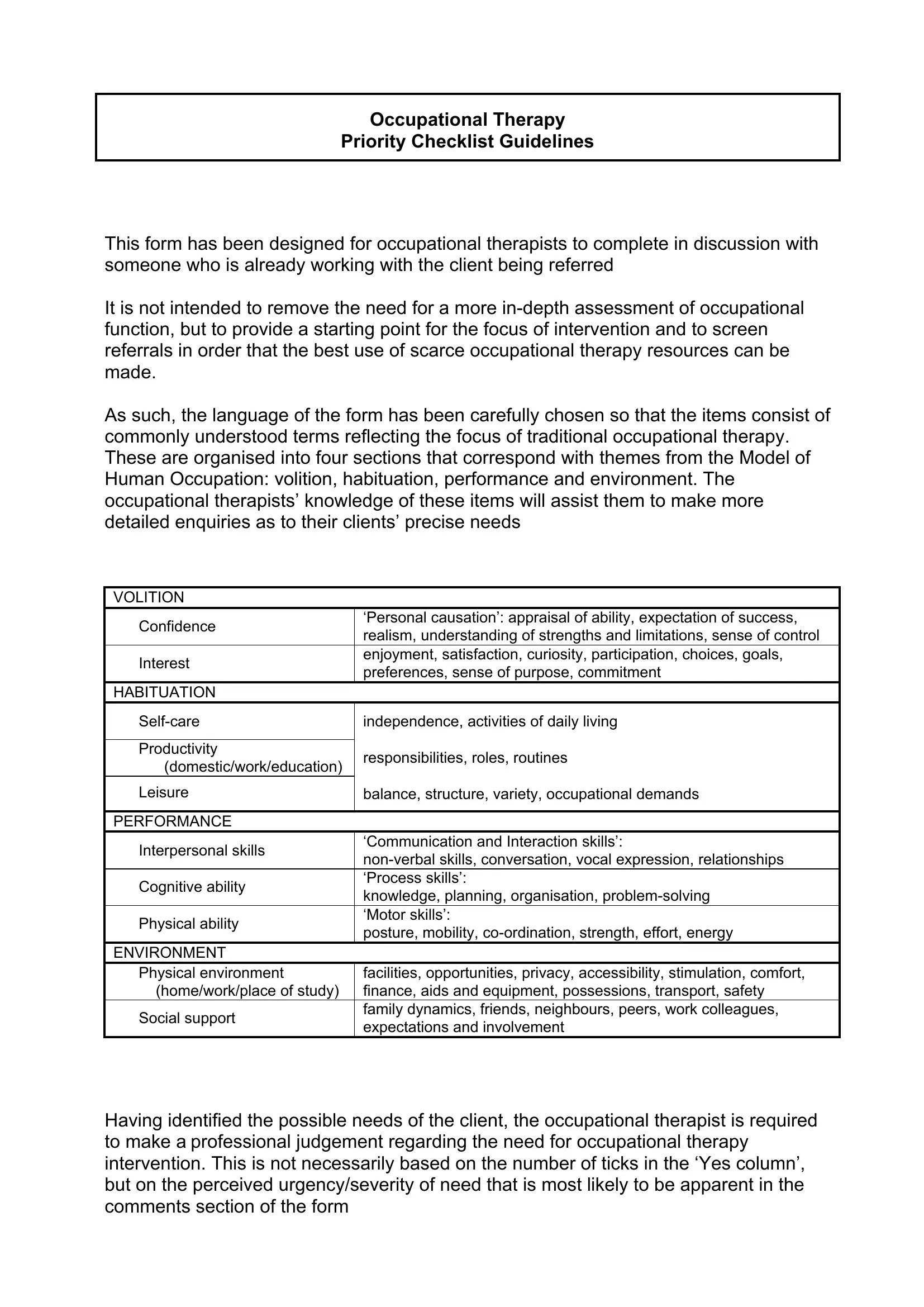
Occupational Therapy
Priority Checklist Guidelines
This form has been designed for occupational therapists to complete in discussion with someone who is already working with the client being referred
It is not intended to remove the need for a more
As such, the language of the form has been carefully chosen so that the items consist of commonly understood terms reflecting the focus of traditional occupational therapy. These are organised into four sections that correspond with themes from the Model of Human Occupation: volition, habituation, performance and environment. The occupational therapists’ knowledge of these items will assist them to make more detailed enquiries as to their clients’ precise needs
VOLITION
Confidence |
‘Personal causation’: appraisal of ability, expectation of success, |
|
realism, understanding of strengths and limitations, sense of control |
||
|
||
Interest |
enjoyment, satisfaction, curiosity, participation, choices, goals, |
|
preferences, sense of purpose, commitment |
||
|
||
HABITUATION |
|
independence, activities of daily living |
||
|
|
|
Productivity |
responsibilities, roles, routines |
|
(domestic/work/education) |
||
|
||
Leisure |
balance, structure, variety, occupational demands |
|
|
|
|
PERFORMANCE |
|
|
Interpersonal skills |
‘Communication and Interaction skills’: |
|
|
||
Cognitive ability |
‘Process skills’: |
|
knowledge, planning, organisation, |
||
|
||
Physical ability |
‘Motor skills’: |
|
posture, mobility, |
||
|
||
ENVIRONMENT |
|
|
Physical environment |
facilities, opportunities, privacy, accessibility, stimulation, comfort, |
|
(home/work/place of study) |
finance, aids and equipment, possessions, transport, safety |
|
Social support |
family dynamics, friends, neighbours, peers, work colleagues, |
|
expectations and involvement |
||
|
Having identified the possible needs of the client, the occupational therapist is required to make a professional judgement regarding the need for occupational therapy intervention. This is not necessarily based on the number of ticks in the ‘Yes column’, but on the perceived urgency/severity of need that is most likely to be apparent in the comments section of the form
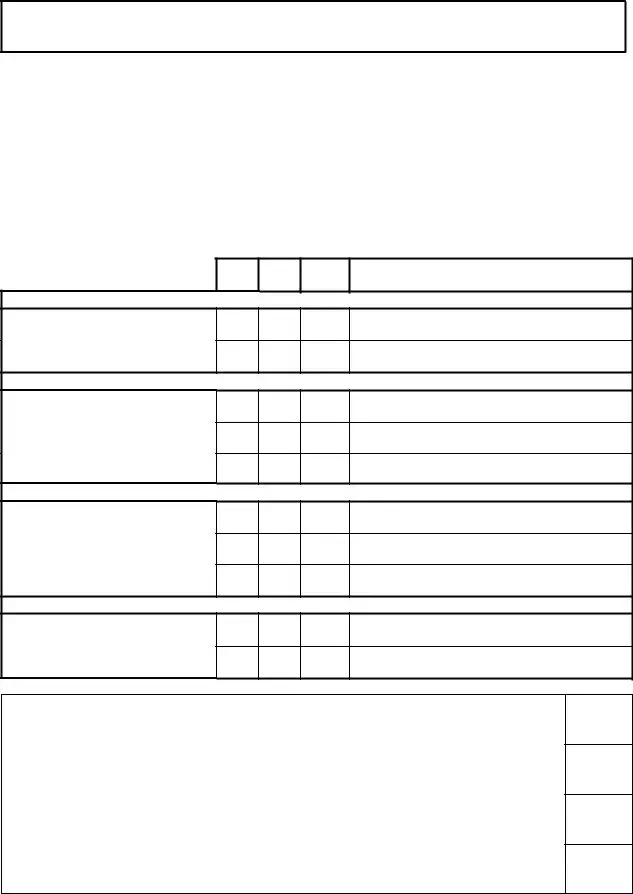
Occupational Therapy Referral
Priority Checklist
Name of client: |
|
Name of worker with whom referral has been |
|
|
…………………………………… |
discussed: |
………………………………………… |
|
|
||
Date of birth: |
____/ ____/ ____ |
Designation: ……………………………………….. |
|
Identity number: …………………………………… |
Date: |
____ / ____ / ____ |
|
Is there any indication that occupational therapy would be useful to help explore or support the following areas of functioning?
Yes No
Don’t know
Comments
MOTIVATION
Confidence
Interest
ROUTINE
Productivity (domestic/work/education)
Leisure
PERFORMANCE SKILLS
Interpersonal skills
Cognitive ability
Physical ability
ENVIRONMENT
Physical environment (home/work/place of study)
Social support
IDENTIFIED NEED FOR OCCUPATIONAL THERAPY
No clear need for OT – no occupational needs identified
Need for minimal intervention/further assessment/consultative OT services to support wellness and/or prevent dysfunction.
Need for OT intervention to restore/improve function
Need for extensive OT intervention to improve function. Referral to
Occupational Therapist: …………………………….. |
Signature: ………………………………………….. |
©2004 Derbyshire Mental Health Services NHS Trust, U.K. / S. Cratchley, S. Parkinson, S. Town, S. Watling, with thanks to A. Lucas & K. Wilshere