OCFS-4659 (Rev. 1/2011)
NEW YORK STATE
OFFICE OF CHILDREN AND FAMILY SERVICES
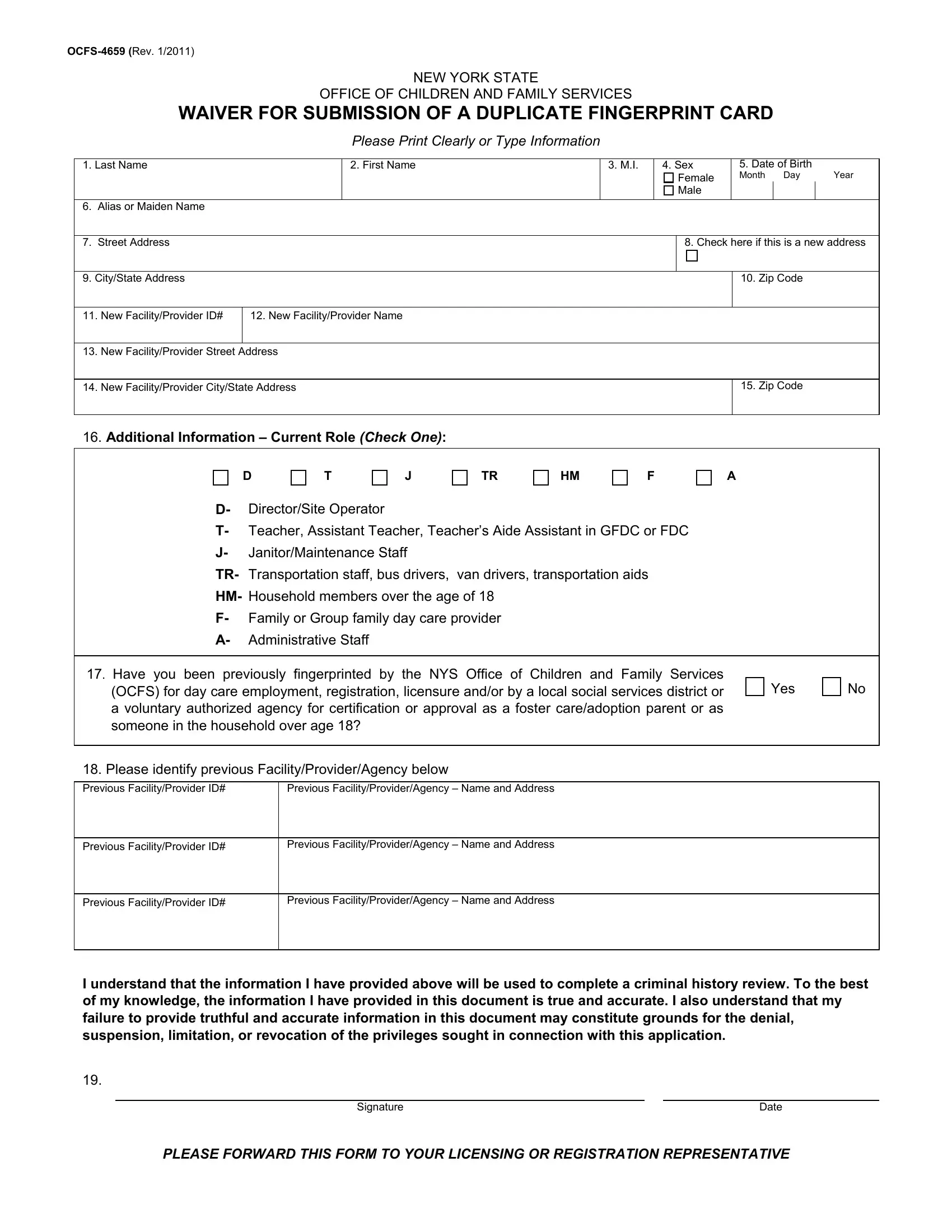
WAIVER FOR SUBMISSION OF A DUPLICATE FINGERPRINT CARD
Please Print Clearly or Type Information
1. |
Last Name |
|
2. First Name |
3. M.I. |
4. Sex |
5. Date of Birth |
|
|
|
|
|
|
|
|
Female |
Month Day |
Year |
|
|
|
|
|
|
|
Male |
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
Alias or Maiden Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7. |
|
Street Address |
|
|
|
|
8. Check here if this is a new address |
|
|
|
|
|
|
|
|
|
9. |
City/State Address |
|
|
|
|
|
10. Zip Code |
|
|
|
|
|
|
|
|
|
|
11. |
New Facility/Provider ID# |
12. New Facility/Provider Name |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
13. |
New Facility/Provider Street Address |
|
|
|
|
|
|
|
|
|
|
|
|
|
14. |
New Facility/Provider City/State Address |
|
|
|
15. Zip Code |
|
|
|
|
|
|
|
|
|
|
|
|
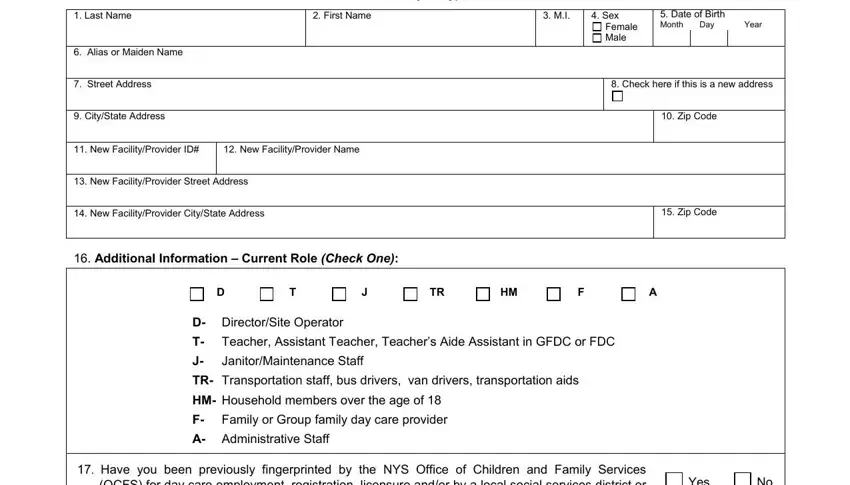
16. Additional Information – Current Role (Check One):
|
D |
T |
J |
TR |
HM |
F |
A |
D- |
Director/Site Operator |
|
|
|
|
|
T- |
Teacher, Assistant Teacher, Teacher’s Aide Assistant in GFDC or FDC |
|
J- |
Janitor/Maintenance Staff |
|
|
|
|
TR- |
Transportation staff, bus drivers, |
van drivers, transportation aids |
|
HM- |
Household members over the age of 18 |
|
|
|
F- |
Family or Group family day care provider |
|
|
|
A- |
Administrative Staff |
|
|
|
|
|
17. Have you been previously fingerprinted by the NYS Office of Children and Family Services |
|
Yes |
|
No |
(OCFS) for day care employment, registration, licensure and/or by a local social services district or |
|
|
a voluntary authorized agency for certification or approval as a foster care/adoption parent or as |
|
|
|
|
someone in the household over age 18? |
|
|
|
|
|
|
|
|
|
|
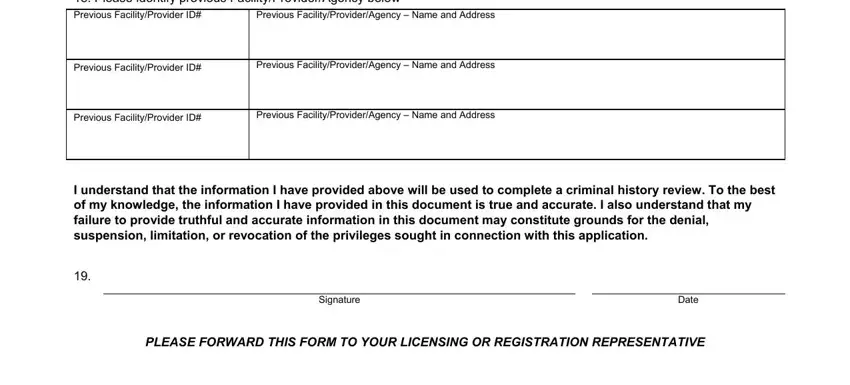
18. Please identify previous Facility/Provider/Agency below |
|
|
|
|
|
|
|
|
|
|
Previous Facility/Provider ID# |
Previous Facility/Provider/Agency – Name and Address |
|
|
|
|
|
|
|
|
|
|
Previous Facility/Provider ID# |
Previous Facility/Provider/Agency – Name and Address |
|
|
|
|
|
|
|
|
|
|
Previous Facility/Provider ID# |
Previous Facility/Provider/Agency – Name and Address |
|
|
|
|
|
|
|
|
|
|
I understand that the information I have provided above will be used to complete a criminal history review. To the best of my knowledge, the information I have provided in this document is true and accurate. I also understand that my failure to provide truthful and accurate information in this document may constitute grounds for the denial, suspension, limitation, or revocation of the privileges sought in connection with this application.
19.
PLEASE FORWARD THIS FORM TO YOUR LICENSING OR REGISTRATION REPRESENTATIVE
OCFS-4659 (Rev. 1/2011)
This form is designed to eliminate the need to submit new fingerprints to the New York State Office of Children and Family Services (NYS OCFS) for the purpose of obtaining a criminal history background check for applicants for day care center/group family day care licenses or employment or volunteers; family day care/school age child care registrations or employment or volunteers. This form is also used for household members over the age of eighteen (18) of applicants who would otherwise be required to submit a fingerprint card.
This form only applies to individuals who have been previously fingerprinted for the purpose described above.
INSTRUCTIONS
PLEASE COMPLETE ALL ITEMS ON FORM
1.Enter applicant’s or household member’s Last Name
2.Enter applicant’s or household member’s First Name
3.Enter applicant’s or household member’s Middle Initial
4.Check “M” for Male or “F” for Female
5.Enter applicant’s or household member’s Date of Birth (mm/dd/yyyy)
6.Alias and/or Maiden Name – Enter any alias or maiden name. Enter any applicable complete name in which the given and /or surname is different than those entered in items 1 thru 3.
7.Enter applicant’s or household members a CURRENT Street Address
8.Check here if this is a new address – The address given in items 7 & 9 is different from address when previously fingerprinted
9.Enter applicant’s or household member’s CURRENT city and state for above address
10.Enter applicant’s or member’s Zip Code
11.New Facility/Provider ID# - The ID # is the license number of the day care facility or provider
12.New Facility/Provider name - The name of the day care facility or provider for which you are now applying
13.New Facility/Provider street address – The address of the day care facility or provider for which you are now applying
14.New Facility/Provider city/ state address- Enter city and state for above address
15.New Facility/Provider zip code- Enter Zip Code
16.Additional Information – Current Role – Check the box that corresponds with the role for which you are currently applying.
17.Have you previously been fingerprinted for Day Care, Foster Care or Adoption purposes through:
The NYS Office of Children and Family Services (OCFS); or
By a local social services district or voluntary authorized agency?
Check “Yes” ONLY if you have been previously fingerprinted by one or more of these organizations. If you check “No”, this form does not apply to you.
18.Previous Facility/Provider/Agency – Enter Facility/Provider/Agency ID# for all locations with which you have previously been affiliated, where you were required to submit a fingerprint card to NYS OCFS in relation to day care, foster care or adoption.
19.This form must be signed and dated by applicant or household member.
This form should only be used if you have already been fingerprinted for child care, foster care, or adoption purposes. This form is meant to be used in lieu of submission of additional fingerprints, and will not be accepted unless fully completed according to the instructions listed above.
UPON COMPLETION: PLEASE FORWARD THIS FORM TO YOUR LICENSING OR REGISTRATION REPRESENTATIVE