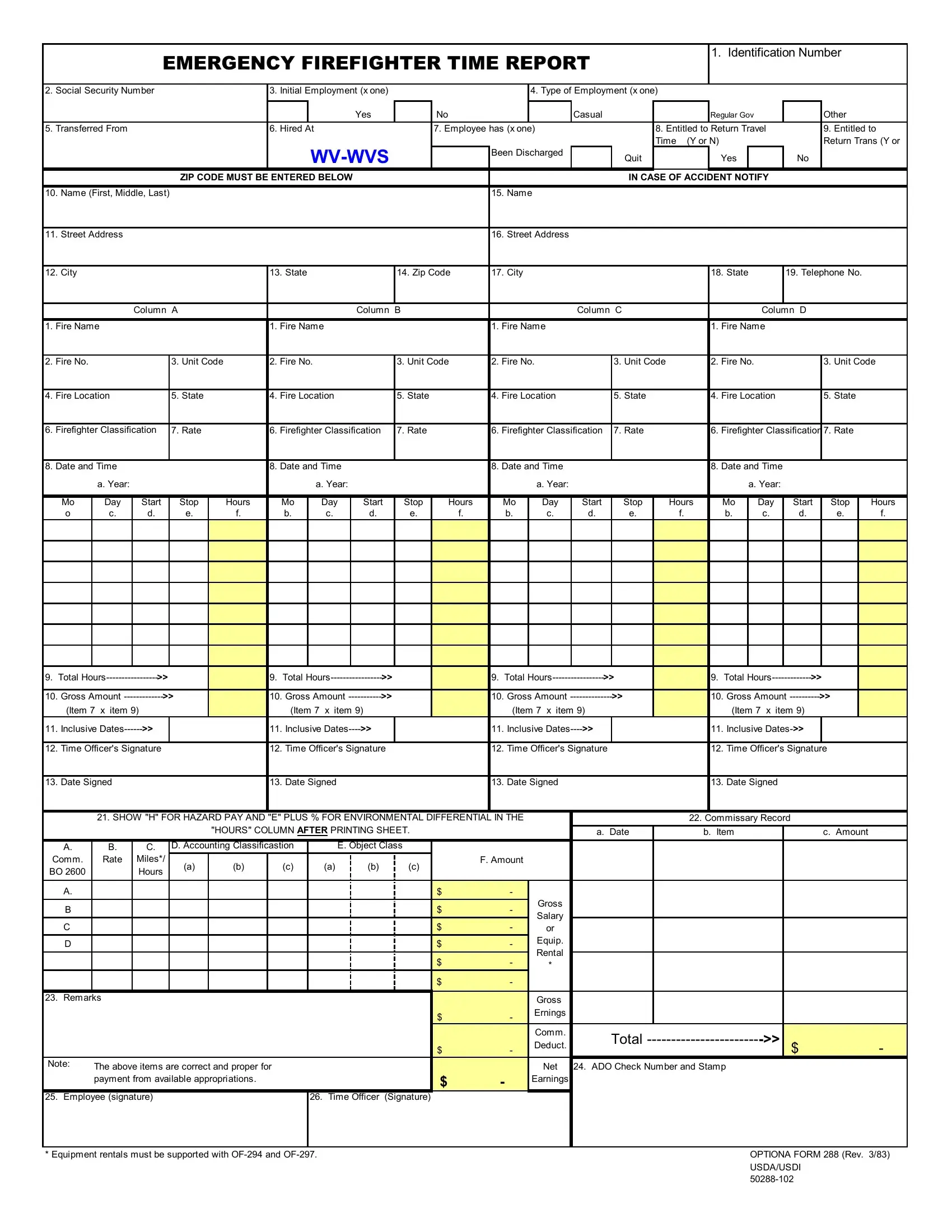
Understanding the intricacies of the OF 288 form, also known as the Emergency Firefighter Time Report, is crucial for professionals and emergency firefighters alike. This form plays a pivotal role in documenting the critical aspects of emergency firefighting employment, encompassing a wide range of information from personal identification details such as Identification Number and Social Security Number to employment-specific data including type of employment, employment status, and detailed accounts of hiring and transfer. Additionally, it addresses crucial financial and operational aspects, involving the recording of fire names, numbers, locations, firefighter classifications and rates, along with comprehensive time reporting covering start and stop times, total hours, gross amounts, and inclusive dates. The form also ensures proper documentation for hazard pay and environmental differential, along with commissary records and accounting classifications to maintain financial accuracy and integrity. Ensuring this form is completed accurately is essential not only for the record-keeping and financial compensation of the firefighters but also for the transparency and efficiency of the emergency firefighting operations themselves.
| Question | Answer |
|---|---|
| Form Name | Of 288 Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | of 288, fillable of 288, form 288, 288 form |
EMERGENCY FIREFIGHTER TIME REPORT
1. Identification Number
2. |
Social Security Number |
|
|
3. |
Initial Employment (x one) |
|
|
|
|
4. Type of Employment (x one) |
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|
|
|
|
Casual |
|
|
Regular Gov |
|
|
Other |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
5. |
Transferred From |
|
|
|
6. |
Hired At |
|
|
|
7. Employee has (x one) |
|
|
|
8. Entitled to Return Travel |
|
9. |
Entitled to |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Time (Y or N) |
|
|
|
|
Return Trans (Y or |
|||
|
|
|
|
|
|
|
|
|
|
Been Discharged |
|
Quit |
|
|
Yes |
|
|
No |
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
ZIP CODE MUST BE ENTERED BELOW |
|
|
|
|
|
|
|
|
IN CASE OF ACCIDENT NOTIFY |
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
10. Name (First, Middle, Last) |
|
|
|
|
|
|
|
|
|
15. Name |
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
11. Street Address |
|
|
|
|
|
|
|
|
|
|
16. Street Address |
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
12. City |
|
|
|
|
13. State |
|
|
14. Zip Code |
17. City |
|
|
|
|
18. State |
|
19. Telephone No. |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Column A |
|
|
|
|
|
Column B |
|
|
|
|
|
Column C |
|
|
|
|
Column D |
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
1. |
Fire Name |
|
|
|
1. |
Fire Name |
|
|
|
1. |
Fire Name |
|
|
|
1. |
Fire Name |
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
2. |
Fire No. |
|
|
3. Unit Code |
|
2. |
Fire No. |
|
|
3. Unit Code |
2. |
Fire No. |
|
|
3. Unit Code |
2. |
Fire No. |
|
|
3. |
Unit Code |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
4. |
Fire Location |
|
5. State |
|
4. |
Fire Location |
|
5. State |
|
4. |
Fire Location |
|
5. State |
|
4. |
Fire Location |
|
5. |
State |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
6. |
Firefighter Classification |
7. Rate |
|
6. |
Firefighter Classification |
7. Rate |
|
6. |
Firefighter Classification |
7. Rate |
|
6. |
Firefighter Classification |
7. |
Rate |
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
8. |
Date and Time |
|
|
|
8. |
Date and Time |
|
|
|
8. |
Date and Time |
|
|
|
8. |
Date and Time |
|
|
|
|
|||||||
|
|
a. Year: |
|
|
|
|
|
|
a. Year: |
|
|
|
|
|
|
a. Year: |
|
|
|
|
|
a. Year: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Mo |
Day |
Start |
Stop |
Hours |
|
Mo |
Day |
Start |
Stop |
Hours |
|
Mo |
Day |
Start |
Stop |
Hours |
|
Mo |
Day |
Start |
Stop |
Hours |
||||
|
o |
c. |
d. |
e. |
f. |
|
b. |
c. |
d. |
e. |
f. |
|
b. |
c. |
d. |
e. |
f. |
|
b. |
c. |
d. |
|
e. |
f. |
|||
9. |
Total |
>> |
|
|
9. |
Total |
>> |
|
|
9. |
Total |
>> |
|
9. |
Total |
>> |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
10. |
Gross Amount |
>> |
|
10. |
Gross Amount |
>> |
|
|
10. |
Gross Amount |
>> |
|
10. |
Gross Amount |
>> |
|
|
|||
|
(Item 7 x item 9) |
|
|
|
|
(Item 7 x item 9) |
|
|
(Item 7 x item 9) |
|
|
(Item 7 x item 9) |
|
|
|
|
||||
11. |
Inclusive |
>> |
|
11. |
Inclusive |
>> |
|
11. |
Inclusive |
>> |
|
11. |
Inclusive |
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
12. |
Time Officer's Signature |
12. |
Time Officer's Signature |
12. |
Time Officer's Signature |
12. |
Time Officer's Signature |
|||||||||||||
13. Date Signed
13. Date Signed
13. Date Signed
13. Date Signed
|
|
21. SHOW "H" FOR HAZARD PAY AND "E" PLUS % FOR ENVIRONMENTAL DIFFERENTIAL IN THE |
|
|
22. Commissary Record |
|
|
||||||||||||
|
|
|
|
|
"HOURS" COLUMN AFTER PRINTING SHEET. |
|
|
a. Date |
b. Item |
|
|
c. Amount |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
A. |
B. |
C. |
D. Accounting Classificastion |
|
|
E. Object Class |
|
|
|
|
|
|
|
|
||||
Comm. |
Rate |
Miles*/ |
(a) |
(b) |
|
(c) |
|
(a) |
(b) |
(c) |
|
F. Amount |
|
|
|
|
|
|
|
BO 2600 |
|
Hours |
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
A. |
|
|
|
|
|
|
|
|
|
|
$ |
- |
|
|
|
|
|
|
|
B |
|
|
|
|
|
|
|
|
|
|
$ |
- |
Gross |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Salary |
|
|
|
|
|
|||
|
C |
|
|
|
|
|
|
|
|
|
|
$ |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
or |
|
|
|
|
|
|||
|
D |
|
|
|
|
|
|
|
|
|
|
$ |
- |
Equip. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Rental |
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
$ |
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
* |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
$ |
- |
|
|
|
|
|
|
23. |
Remarks |
|
|
|
|
|
|
|
|
|
|
|
Gross |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
- |
Ernings |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Comm. |
Total |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
$ |
- |
Deduct. |
|
$ |
- |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
Note: |
The above items are correct and proper for |
|
|
|
|
|
|
|
Net |
24. ADO Check Number and Stamp |
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
payment from available appropriations. |
|
|
|
|
|
$ |
- |
Earnings |
|
|
|
|
|
||||
25. |
Employee (signature) |
|
|
|
|
26. |
Time Officer |
(Signature) |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
* Equipment rentals must be supported with |
|
|
|
|
|
|
|
OPTIONA FORM 288 (Rev. 3/83) |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
USDA/USDI |
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||