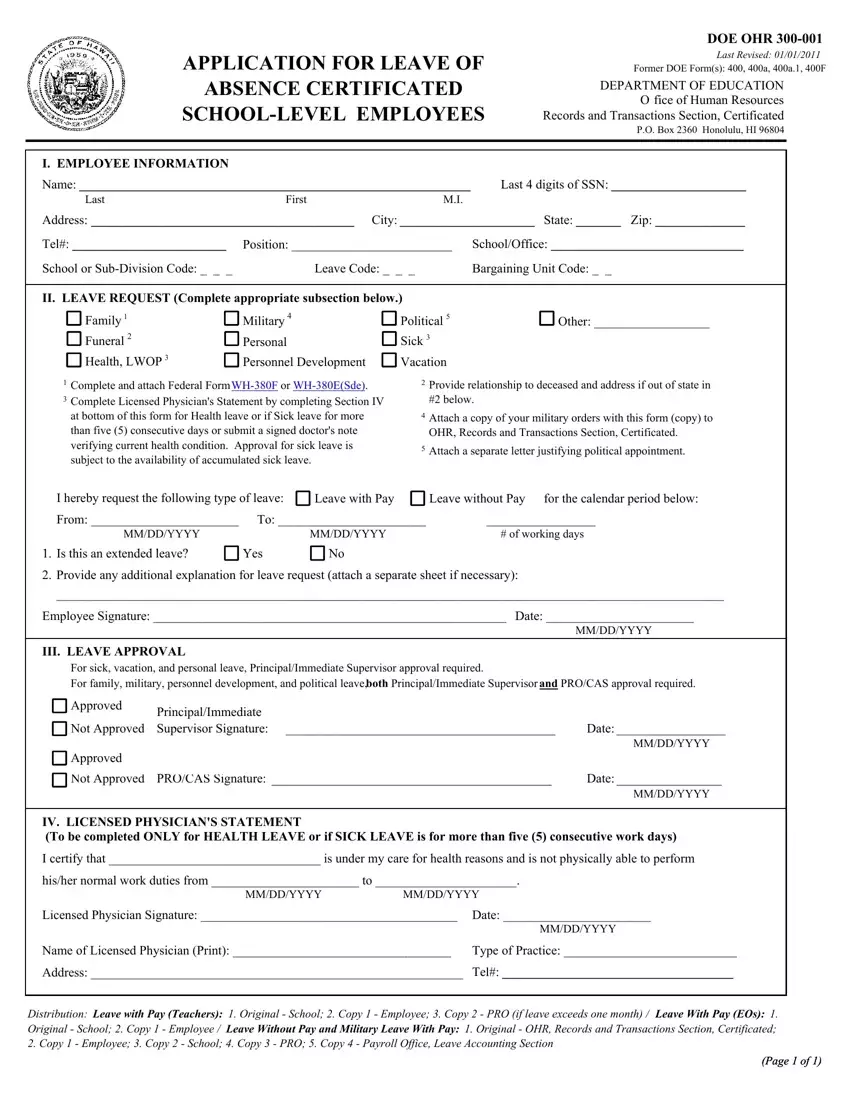
Understanding the complexities of requesting leave as a certificated school-level employee within the Department of Education necessitates a thorough examination of the Ohr 400A form. Last revised on January 1, 2011, and evolving from previous forms including the 400, 400a, 400a.1, and 400F, this document serves as a critical tool for employees seeking various types of leave, including but not limited to family, military, funeral, personal sick, health, leave without pay (LWOP), personnel development, and vacation leave. Applicants are required to provide essential employee information, details of the leave request, and, depending on the nature of the leave, additional documentation such as a physician's statement for health-related absences or military orders for military leave. The process also entails the necessity of approval from direct supervisors or, in some cases, higher authorization from Principal/Immediate Supervisor and PRO/CAS for certain types of leave. This form not only outlines the procedure for requesting leave but also stipulates the distribution of the completed forms, ensuring a comprehensive approach to managing leave requests effectively and efficiently. As such, for educators and administrative staff navigating their rights and responsibilities regarding leave, understanding the components and stipulations of the Ohr 400A form becomes a vital aspect of their professional lives.
| Question | Answer |
|---|---|
| Form Name | Ohr Form 400A |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | tseas hawaii, hawaii doe leave of absence form, hawaii doe leave of absence, maritime leave request form |
