|
|
|
|
|
|
, |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
, |
"" |
|
|
|
|
|
|
|
|
|
|
|
|
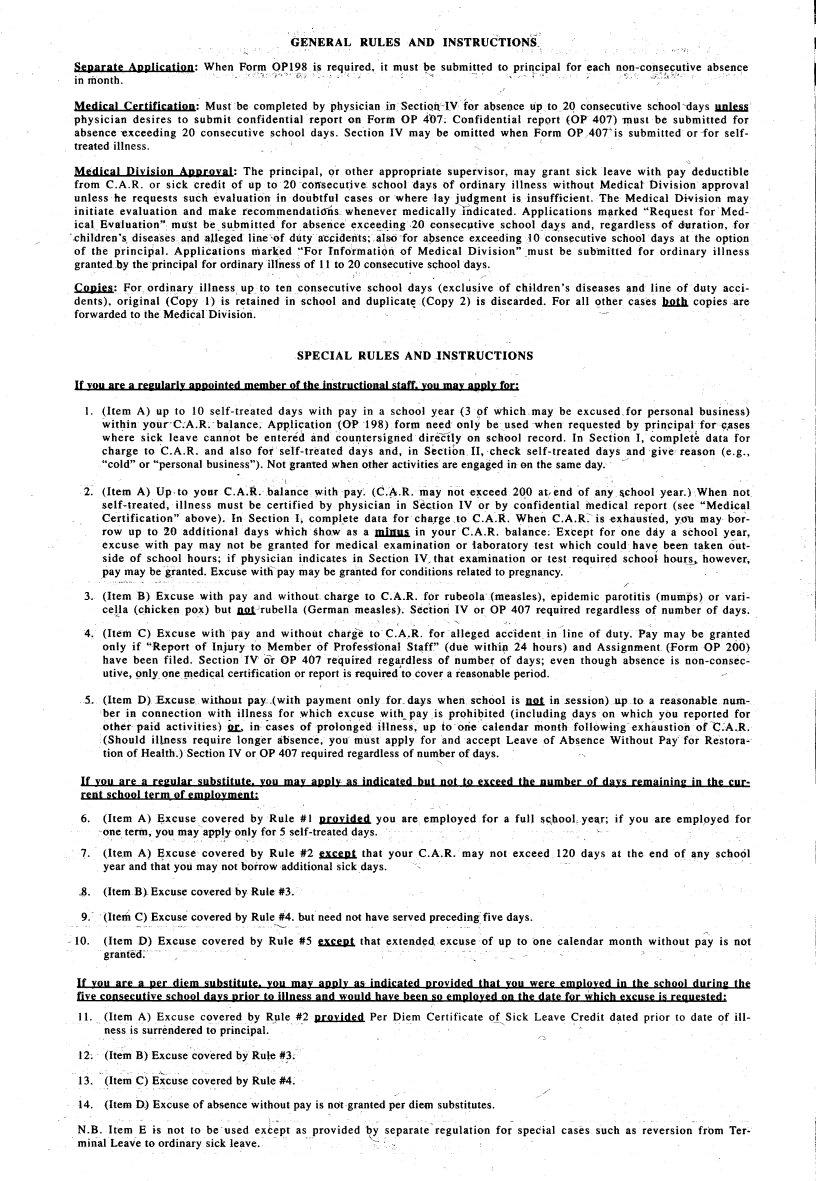
GENERAL |
RULES AND INSTRUCTIONS_, |
|
|
|
|
|
|
|
~eRara&e |
ARRlica&ign: |
When |
~~~9~1~~i,s~eq~ired, |
'" |
it |
must \i; |
submitted |
to |
pr!qc ~pal, |
for each nl?n-co~~~~,,';Itlve absen<::;e |
mmonth. |
|
|
|
-, |
,"- |
|
|
|
,-' |
|
|
|
|
'0"";"" |
|
|
|
|
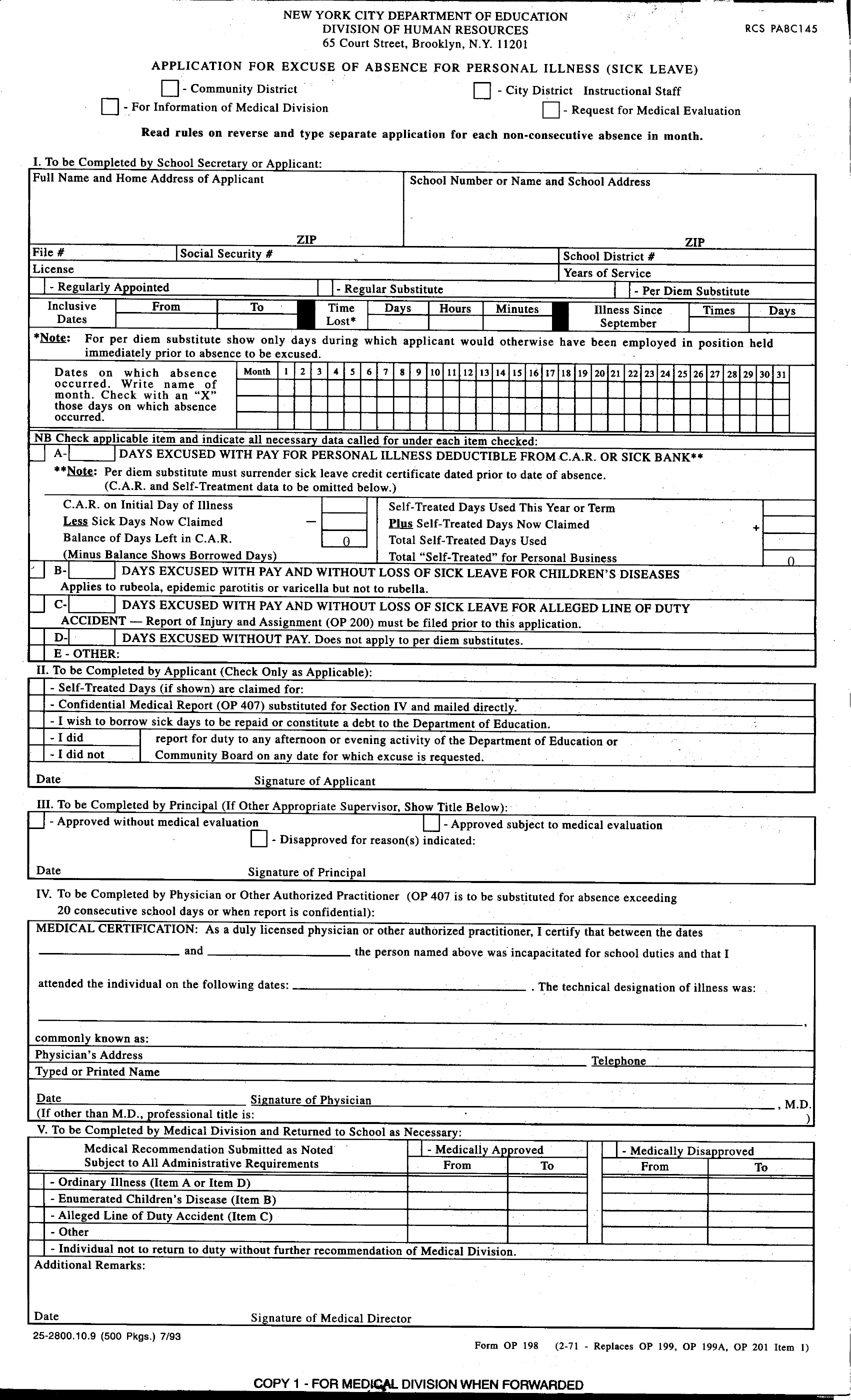
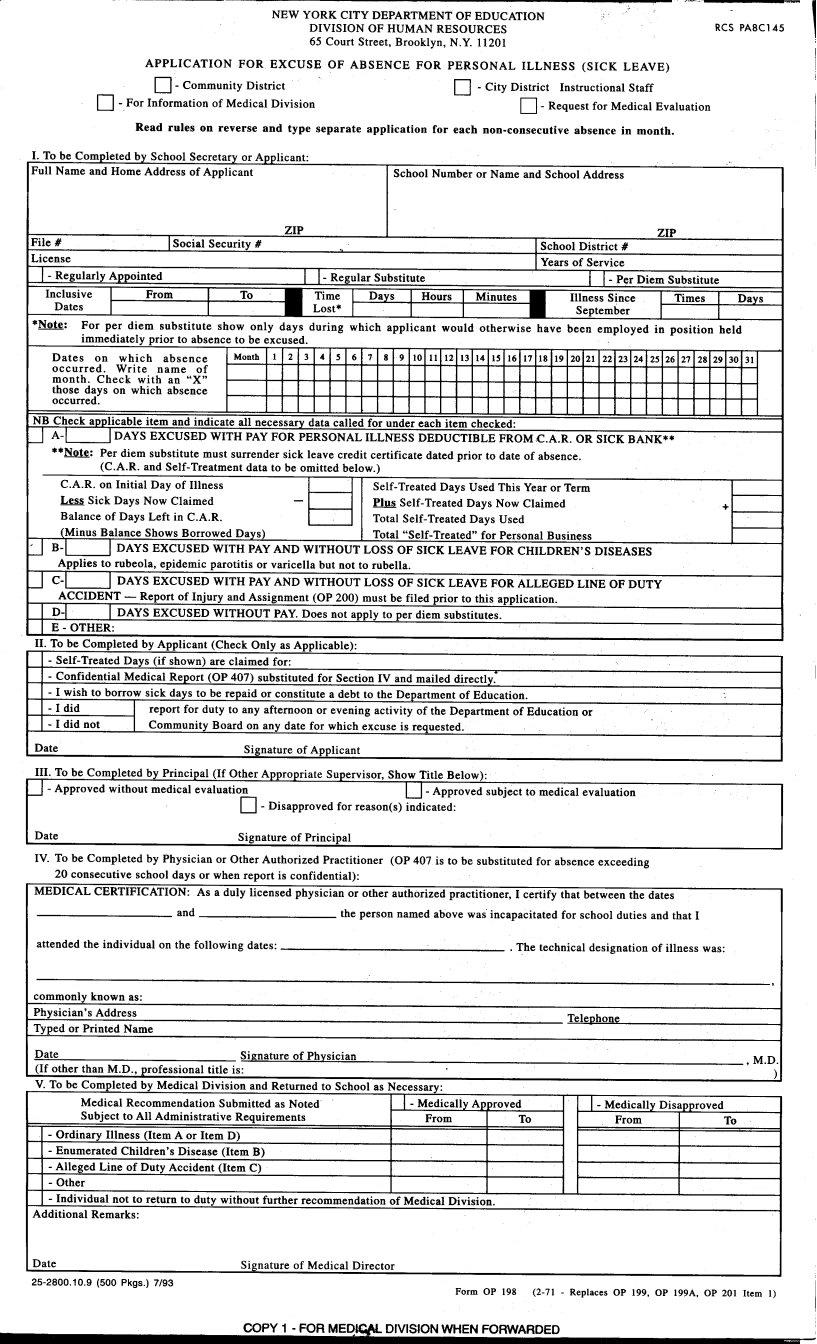
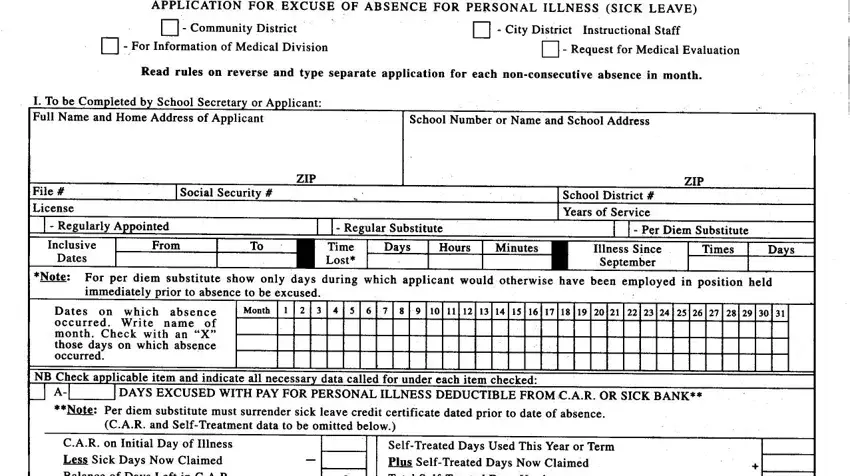
Medical |
Certification: |
Must |
be completed |
by |
physician |
in |
SectiQil:~.lVfQr abseJ)ce up |
to.2<1 cons~~utive |
school 'days 1IDlw" |
physician |
desires |
10 |
submit confidential |
report |
on Form OP 4"07; Confidential |
report |
(OP 401) |
~ust be |
submitted for |
absence-exceeding |
20 |
consecutive |
~chool |
days. |
Section IV |
may |
be omitted |
when Form OP40Tis |
submitted or -for self- |
treated illness. |
|
|
|
|
|
|
|
|
|
|
|
|
" |
|
|
|
|
|
|
|
Medical |
Division |
AoRrllval: |
The |
principal, |
Qr other |
appropriate |
supervisor, |
may "grant sick |
leave |
with |
pay |
deductible |
from C.A.R. or |
sick |
credit |
of up |
to 20 coniSecutive schoo" |
days |
of ordinary |
illness |
witltOQt |
MedicatDivision |
approval |
unless he requests such evaluation in doubtful cases or "where lay judgment is jnS11fficient. The Medical Divitiion may
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
initiate evaluation |
and maketecommendatidhs |
whenever |
medicallylndicated. |
Applications |
m!1rked "Request |
for |
Med- |
icaIEvaluation" |
must |
be. submitted |
for |
abs;ericeexce~qing20 |
c~nsec~tive |
school |
da):s |
and, |
regardtess |
"of |
duration,for |
',chil"dren 's:"di~~asesapd |
.aUe.ged li~'of |
dutya'C~idents;;~IS:<5 |
for a!>s:nce e~c:e?ing i 0 |
cons~cutive ,schoot |
days |
.at the .option |
of the princIpal. |
ApplIcatIons |
mark;ed "For TnformatIQn of MedIcal DIvIsIon" ,must be submItted for ordinary Illness |
granted by the principal forotdinary iUness of 1 t to 20 consecutive S1;hooldays. |
|
|
|
|
|
|
|
|
CoRi~s: For ordi~ary |
i.llness |
up to |
ten |
consecutivesch"ool |
days |
(exclusive |
of children's |
diseas"es ijnd |
line |
of |
duty |
acci- |
dents), originat (Copy 1) is retained in schqol and duplicat~ (Copy 2) is discarded. For all other cases bJ!1h copies are
forwarded to the MedicalDivision. |
~ |
SPECIAL RULES AND INSTRUCTIONS
If IOU are a re~ularlI aRRointed member oftbe instructional 5taff.Iou maI a~RII for:
I.(Item A) up to 10 self-tre~ted days with pay in a school year (3 pf Which may be excused for personal business)
within ~our'C:A;R.ba}ance; AP1?Jtcation (OP }98} forql?e~ only be;used -wheff request~.d by pri~cipal,fot~.as"es where sick leave cannot be entered and co~l:Itersigned dIrectly on school record. In SectIon I, complete data for
charge to C.A.R. and also for self-treated days and, in Stction II, check self-treated days and "give reason (e.g..
:'cold" or "personal business"). Not :granted WRenother activities are engaged in en the same day; -~
2.(Item A) Up. to yollr C.A.R.balance ~ith pay.. (C..&.R.may not e~ceed 290 attend of any&chool year.);W"hen not
self-treated, illness must be certified by physician in S~tion IV or by collfidential i:nedical report (see "Medk!\l
Certification" above). In Section I; compl_et~ data for charge,to C.A.R.. When C.A.R: is ~xha.usied, yl:ru maybor-
"
row up to 10 additional days which sho.w a~ a ~ in your C.A.R. balance; Except for one day a school year,
excuse with pay may not be granted for medical examination ot i~boratory 1est which could hav~ been; taken out- side of school hours; if physician indicates in Section IV/ that examination or test required school hQut:~ however.. pay may be granted. Excuse witl1pay may be granted for conditions related to pregnancy.
./
J. (Item B) Excuse with pay and without charge to C.A.R. for rubeola (measles), epidemic parotitis (mumps) or vari-
cetla (Cbick~!l po~) but Wlj;Jrubella {German measl~s). Section.IV or OP 407 required regardless of number of days."
"4, (Item C) Excuse with pay and without charge toC.A.R. for alleged acci"dent in line of duty." Pay may be granted
only if "Report of In~ryto Member of Profemonal Stlicff." (due withi~ 24 hours) and Assignment (Form OP 200) have been filed.. Section W'Of OP 407 requir.ed regardless of numbe~ of days; even though absence is non-consec-
utive, 9!lIYQnerncedi"al certification or report is required'tocover a reasonable period.
5/ {Item D) Excuse without pay ,(with payment only for days when;school is WIj; in .session) up to a reasonabl.enum-
ber in co,nneC"tion wit~ illnes.s for Which excuse with- pay is prQhibited (including days on which you reported for
other paid activiiies)St;l., in-cases of prolonged il.lness; up to one calendar month follQwingexhaustion of-:C:A,R.. (Should iltDess require longer aDsence, you must apply for and accept Leave of Ab~ence Without Pay "for Restora.
tion of" Health.) Section IV or OP 407 required regardless of number of days.
"
rent school term- of emgloIment:
6.(Item A) ~xcusecovered by Rule #1 R[ovided you are emptoyed for a full &~,~90t,yellr; if you are emplpyed for
oneteftn, you may appty only |
for 5 self-treated days. |
' |
"" |
;" |
"" |
|
7.,,(It~mA) ~xcuse covered by ,,~ule #2 ~ that yourC.A.R. may not exceed 120 days at the end of~ny scho?1
year and that you |
may not |
borrow additi9nal |
sick days. |
' |
|
|
~. (ItemB}Excuse covered by Rule #3; |
|
|
|
|
9: (Itelfi C) Excuse covered |
by Rule #4. but need not have served preceding |
five |
days. |
|
|
"'- |
|
|
" |
~ |
~10. (Item D) Excuse |
covered by Rule #5 ~ |
that |
extend~d,excQ~e |
of |
up to one calendar month without pay is not |
granted: |
|
|
|
" |
|
|
"
11.(Item A) Excuse covered by RJIle #2 Rrovided Per Diem Certificate of Sick Leave Credit dated prior to date of il.l-
ness is surrendered to principal..~,
/0
11; {Item B) Excuse c9vered by Rute #3;.
"~
13.(Item C) Excuse covered by Rule #4.
"
14.(Item D.) Ex{)use of absence without pay is ndtgrantedper di~ substitutes.
" ,
N.B. Item E is not to be used ex~ept as provided by separate'regulation for special cases such as reveTsion from Ter- |
" |
" |
minal Leave to ordinary sick l~~ve. |
~ |