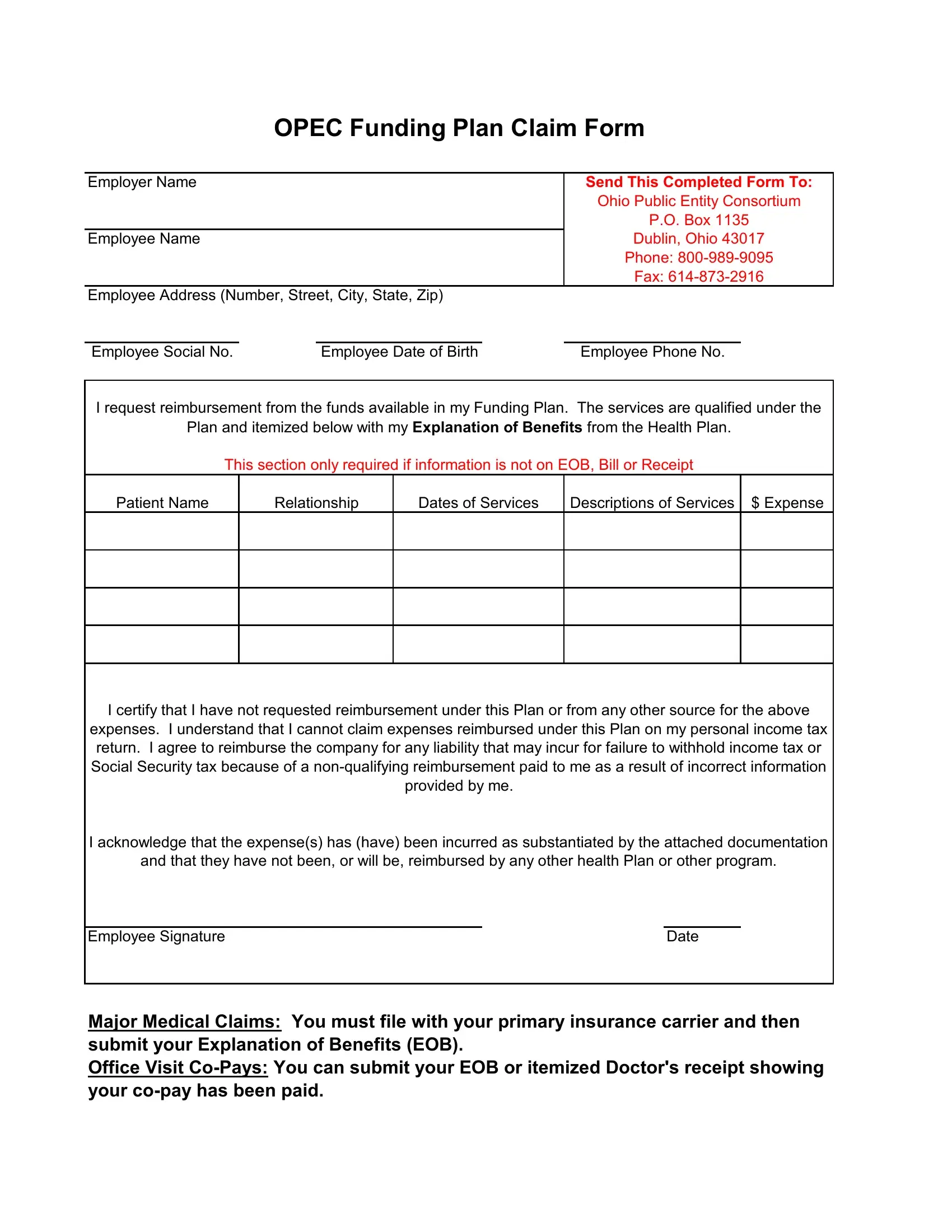
The OPEC Funding Plan Claim Form serves as a crucial document for employees seeking reimbursement for qualified health expenses through the Ohio Public Entity Consortium. It requires comprehensive information, including the employer and employee names, addresses, social security numbers, dates of birth, and contact details, to ensure accurate processing. This form allows eligible employees to request funds from their funding plan for expenses that are supported by their health plan, specifically detailing necessary services that are eligible under the plan. Those filing the claim must include documentation such as an Explanation of Benefits (EOB), bills, or receipts for the services rendered, clearly itemizing dates of services, descriptions, and expenses incurred. Additionally, the form requires claimants to certify that they have not and will not seek reimbursement for these expenses from any other source, and understand the tax implications of their reimbursements. Importantly, for major medical claims, the procedure necessitates that claims are first submitted to the primary insurance carrier, with this form and the EOB following thereafter. Office visit co-payments are eligible for direct submission, provided that documentation verifies the co-payment has been fulfilled. The meticulous completion of this form, backed by the required documentation and adherence to the guidelines, facilitates the reimbursement process, ensuring that employees can efficiently and effectively manage their health-related financial matters.
| Question | Answer |
|---|---|
| Form Name | Opec Funding Plan Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | reimbursed, opec full form, opec funding plan claim form, Ohio |
|
OPEC Funding Plan Claim Form |
||||
|
|
|
|
|
|
Employer Name |
|
|
|
Send This Completed Form To: |
|
|
|
|
|
Ohio Public Entity Consortium |
|
|
|
|
|
P.O. Box 1135 |
|
Employee Name |
|
|
|
Dublin, Ohio 43017 |
|
|
|
|
|
Phone: |
|
|
|
|
|
Fax: |
|
Employee Address (Number, Street, City, State, Zip) |
|
|
|
||
|
|
|
|
|
|
Employee Social No. |
|
Employee Date of Birth |
|
Employee Phone No. |
|
I request reimbursement from the funds available in my Funding Plan. The services are qualified under the
Plan and itemized below with my Explanation of Benefits from the Health Plan.
This section only required if information is not on EOB, Bill or Receipt
Patient Name
Relationship
Dates of Services
Descriptions of Services
$ Expense
I certify that I have not requested reimbursement under this Plan or from any other source for the above expenses. I understand that I cannot claim expenses reimbursed under this Plan on my personal income tax return. I agree to reimburse the company for any liability that may incur for failure to withhold income tax or Social Security tax because of a
I acknowledge that the expense(s) has (have) been incurred as substantiated by the attached documentation
and that they have not been, or will be, reimbursed by any other health Plan or other program.
Employee Signature |
Date |
Major Medical Claims: You must file with your primary insurance carrier and then submit your Explanation of Benefits (EOB).
Office Visit