Are you authorized to receive funding from the Organization of Petroleum Exporting Countries (OPEC)? If so, you’ve come to the right place. This blog post will provide an overview of OPEC's funding plan, explain who is eligible for assistance and guide you through the claim forms needed to collect your payment. With a clear understanding of how this program works, applying for funds can be simple and straightforward. Read on to learn more about the funding options available under OPEC's Claim Form program.
| Question | Answer |
|---|---|
| Form Name | Opec Funding Plan Claim Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | reimbursed, opec full form, opec funding plan claim form, Ohio |
|
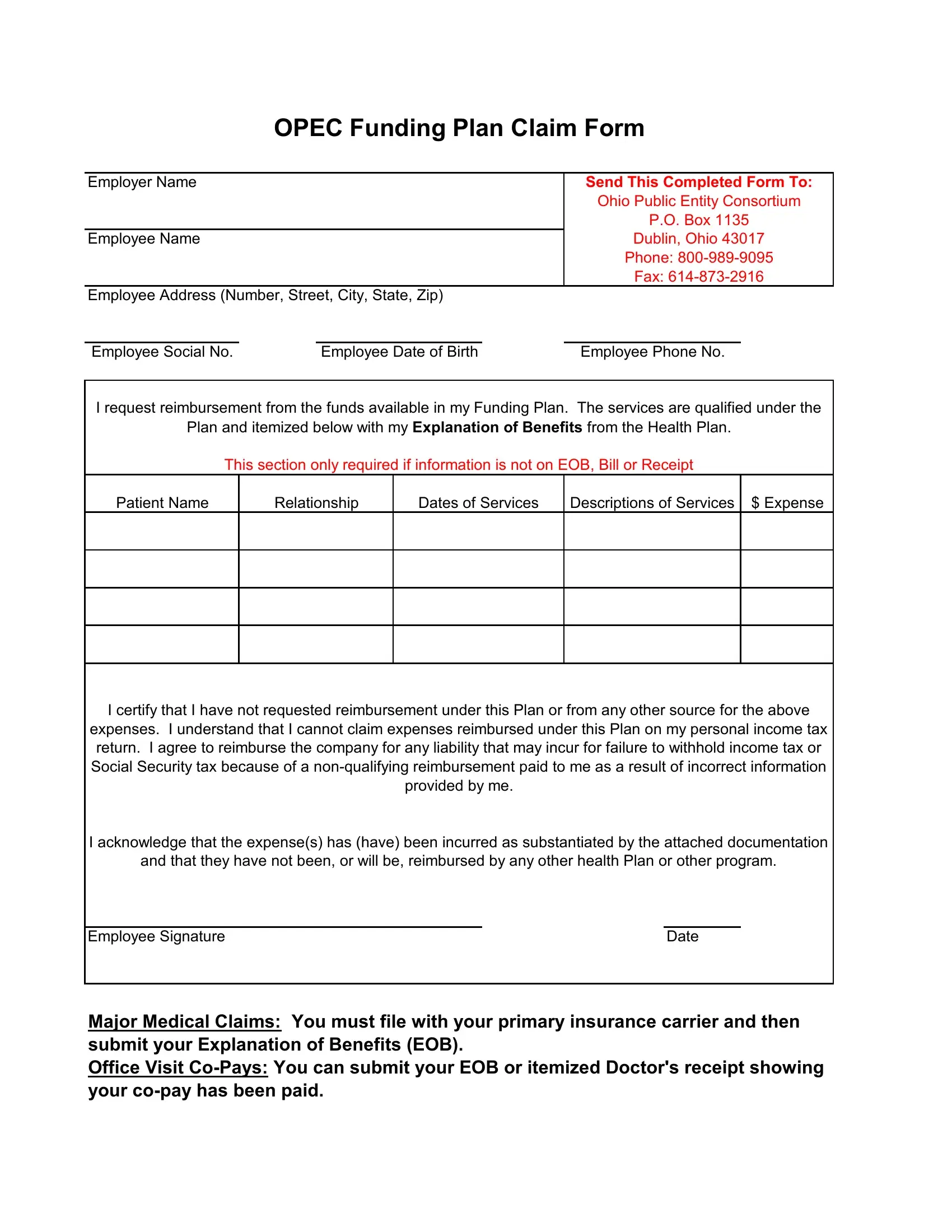
OPEC Funding Plan Claim Form |
||||
|
|
|
|
|
|
Employer Name |
|
|
|
Send This Completed Form To: |
|
|
|
|
|
Ohio Public Entity Consortium |
|
|
|
|
|
P.O. Box 1135 |
|
Employee Name |
|
|
|
Dublin, Ohio 43017 |
|
|
|
|
|
Phone: |
|
|
|
|
|
Fax: |
|
Employee Address (Number, Street, City, State, Zip) |
|
|
|
||
|
|
|
|
|
|
Employee Social No. |
|
Employee Date of Birth |
|
Employee Phone No. |
|
I request reimbursement from the funds available in my Funding Plan. The services are qualified under the
Plan and itemized below with my Explanation of Benefits from the Health Plan.
This section only required if information is not on EOB, Bill or Receipt
Patient Name
Relationship
Dates of Services
Descriptions of Services
$ Expense
I certify that I have not requested reimbursement under this Plan or from any other source for the above expenses. I understand that I cannot claim expenses reimbursed under this Plan on my personal income tax return. I agree to reimburse the company for any liability that may incur for failure to withhold income tax or Social Security tax because of a
I acknowledge that the expense(s) has (have) been incurred as substantiated by the attached documentation
and that they have not been, or will be, reimbursed by any other health Plan or other program.
Employee Signature |
Date |
Major Medical Claims: You must file with your primary insurance carrier and then submit your Explanation of Benefits (EOB).
Office Visit