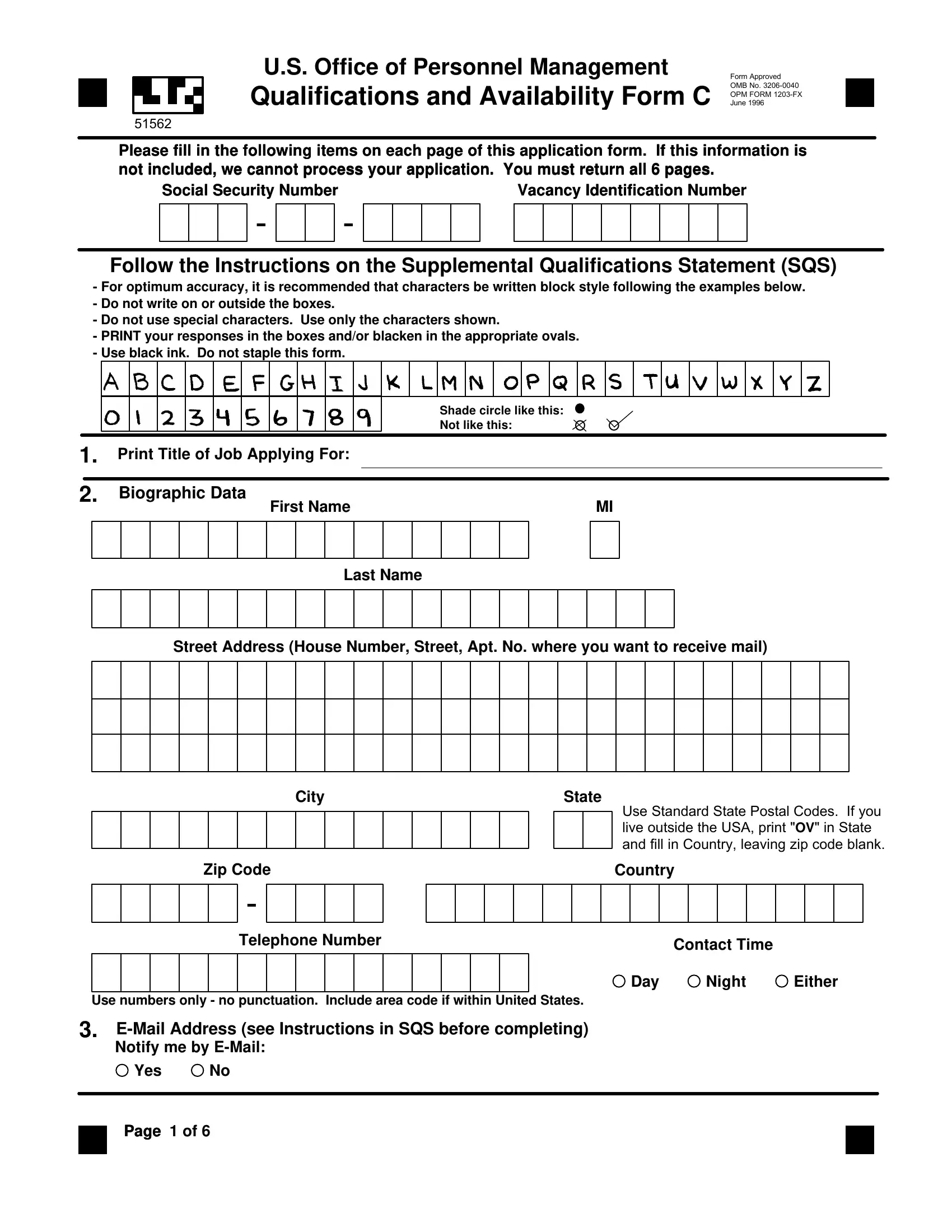
The U.S. Office of Personnel Management (OPM) Form C, officially known as the Qualifications and Availability Form C 51562, serves as a critical component for candidates seeking federal employment. Approved by the OMB with a designation No. 3206-0040, and last updated in June 1996, this comprehensive form demands meticulous attention to detail across its six pages. Applicants are required to provide a wealth of information, ranging from basic biographic data and work information to more detailed inquiries about employment availability, citizenship status, and even veteran preference claims. Additionally, the form delves into aspects such as languages spoken, grade levels being applied for, and specific job preferences, making it a pivotal part of the federal employment application process. Not only does the Form C facilitate a structured way for applicants to present their qualifications and availability, but it also ensures that hiring agencies have a consistent basis for evaluating potential candidates. Completing the form accurately is vital; any omitted information can halt the application process, making it indispensable for candidates to follow the provided instructions carefully. The emphasis on printing responses and using black ink, alongside specific instructions for entering various types of information, underscores the form's importance in the meticulous federal hiring landscape.
| Question | Answer |
|---|---|
| Form Name | Opm Form C |
| Form Length | 7 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 1 min 45 sec |
| Other names | how to opm form c, qualifications formc, availability c, instructor qualifications form c |
U.S. Office of Personnel Management
Qualifications and Availability Form C
51562
Form Approved
OMB No.
OPM FORM
June 1996
Please fill in the following items on each page of this application form. If this information is not included, we cannot process your application. You must return all 6 pages.
Social Security Number |
Vacancy Identification Number |
- -
Follow the Instructions on the Supplemental Qualifications Statement (SQS)
-For optimum accuracy, it is recommended that characters be written block style following the examples below.
-Do not write on or outside the boxes.
-Do not use special characters. Use only the characters shown.
-PRINT your responses in the boxes and/or blacken in the appropriate ovals.
-Use black ink. Do not staple this form.
Shade circle like this: |
Not like this: |
1. Print Title of Job Applying For:
2. |
Biographic Data |
|
MI |
|||||||||||||||
|
|
|
|
|
|
|
|
First Name |
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Last Name
Street Address (House Number, Street, Apt. No. where you want to receive mail)
City |
State |
Use Standard State Postal Codes. If you live outside the USA, print "OV" in State and fill in Country, leaving zip code blank.
Zip Code |
Country |
|
|
- |
|
|
|
Telephone Number |
Contact Time |
|
|
|
|
||
|
Day |
Night |
Either |
Use numbers only - no punctuation. Include area code if within United States.
3.
Notify me by
Yes No
Page 1 of 6
51562
Please fill in the following items on each page of this application form. If this information is not included, we cannot process your application. You must return all 6 pages.
Social Security Number |
Vacancy Identification Number |
-
-
4. Work Information ( If Applicable ) |
Place of Employment |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work Address |
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work City |
|
Work State |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Use Standard State Postal Codes. If you |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
work outside the USA, print "OV" in State |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
and fill in Country, leaving zip code blank. |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
Work Zip Code |
|
|
|
|
Work Country |
|||||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
- |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Work Telephone Number |
|
|
|
|
|
Extension |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Use numbers only - no punctuation. Include area code if within United States.
5. Employment Availability - Are you available for:
A. Full Time Employment |
Y N |
|
|
|
|
B. Part Time Employment of |
|
|
|
|
|
|
|
|
|
|
|
C. Temporary Employment Lasting |
|
|
|
|
|
|
|
|
|
|
|
D. Jobs Requiring Travel Away from |
|
|
home for |
|
|
|
|
|
|
|
|
E. Other Employment Questions (see instructions)
Y N |
Y N |
Question 1. |
Question 4. |
Question 2. |
Question 5. |
Question 3. |
Question 6. |
6. |
Citizenship |
|
|
|
Are you a citizen of the United States? |
||
|
Yes |
No |
|
7. |
Background Information |
||
|
(see Instructions in SQS before completing) |
||
|
|
Y N |
Y N |
|
Question 1. |
|
Question 4. |
|
Question 2. |
|
Question 5. |
|
Question 3. |
|
Question 6. |
8. |
Other Information |
|
|
|
(see Instructions in SQS before completing) |
||
|
A. Gender |
Male |
Female |
B.Date of Birth (MM/DD/YYYY)
/ /
Page 2 of 6
51562
Please fill in the following items on each page of this application form. If this information is not included, we cannot process your application. You must return all 6 pages.
Social Security Number |
Vacancy Identification Number |
-
-
9. Languages |
|
|
|
|
|
|
|
|
|
|
|
|
10. Lowest Grade |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
11. Miscellaneous Information
12. Special Knowledge |
|
|
|
|
|
|
|
|
|
|
|
|
13.Test Location |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
14. |
Veteran Preference Claim |
|
|
|
|
When entering dates in the following fields, |
|||||||
|
|
|
|
please use the format: MM/DD/YYYY |
|
||||||||
|
|
|
|
|
|
|
|
|
|||||
No Preference Claimed |
|
|
|
|
15. Dates of Active Duty - Military Service |
||||||||
|
|
|
|
|
|
|
|
||||||
5 Points Preference Claimed |
|
|
|
Skip if No Veteran Preference Claimed in Block 14 |
|||||||||
|
|
|
|
|
|
|
|
|
|||||
|
10 Point Preference - You must submit a |
|
From: |
|
/ |
/ |
|
|
|||||
|
completed Standard Form 15. |
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
||||
10 Points Preference Claimed |
|
|
|
To: |
|
/ |
/ |
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|||
|
( award of a Purple Heart or noncompensable |
|
|
|
|
|
|
||||||
|
|
|
|
|
16. Availability Date |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|||
10 Points Compensable Disability Preference Claimed |
|
/ |
|
/ |
|
|
|||||||
|
( disability rating of less than 30% ) |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||
10 Points Other |
|
|
|
|
|
17. Service Computation Date |
|
|
|||||
|
|
|
|
|
|
/ |
|
/ |
|
|
|||
|
( wife, widow, husband, widower, mother |
|
|
|
|
|
|
||||||
|
preference claimed ) |
|
|
|
|
|
18. Other Date |
|
|
|
|
||
10 Points Compensable Disability Preference Claimed |
|
|
|
|
|||||||||
|
/ |
|
/ |
|
|
||||||||
|
( disability rating of 30% or more ) |
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
||||
19. Job Preference |
|
|
|
|
|
|
|
|
|
|
|
||
1 |
6 |
11 |
16 |
21 |
26 |
31 |
36 |
41 |
46 |
51 |
56 |
61 |
66 |
2 |
7 |
12 |
17 |
22 |
27 |
32 |
37 |
42 |
47 |
52 |
57 |
62 |
67 |
3 |
8 |
13 |
18 |
23 |
28 |
33 |
38 |
43 |
48 |
53 |
58 |
63 |
68 |
4 |
9 |
14 |
19 |
24 |
29 |
34 |
39 |
44 |
49 |
54 |
59 |
64 |
69 |
5 |
10 |
15 |
20 |
25 |
30 |
35 |
40 |
45 |
50 |
55 |
60 |
65 |
70 |
|
Page |
3 of 6 |
|
|
|
|
|
|
|
|
|
|
|
51562
Please fill in the following items on each page of this application form. If this information is not included, we cannot process your application. You must return all 6 pages.
Social Security Number |
Vacancy Identification Number |
-
-
20. |
|
Occupational Specialties |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
1 |
2 |
|
|
|
|
|
|
3 |
|
|
4 |
|
5 |
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
7 |
|
|
|
|
|
|
8 |
|
|
9 |
|
10 |
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
21. |
|
Geographic Availability |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
9 |
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
10 |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22. Indicate if you are requesting consideration for either the:
Career Transition Assistance Plan (CTAP)
Interagency Career Transition Assistance Plan (ICTAP)
23. Job Related Experience
(see Instructions in SQS before completing)
Years: |
|
|
Months: |
|
|
|
|
24.Personal Background Information
(see Instructions in SQS before completing)
1 |
11 |
2 |
12 |
3 |
13 |
4 |
14 |
5 |
15 |
6 |
16 |
7 |
17 |
8 |
18 |
9 |
19 |
10 |
20 |
Page 4 of 6
25. Occupational Questions
51562
Please fill in the following items on each page of this application form. If this information is not included, we cannot process your application. You must return all 6 pages.
Social Security Number |
Vacancy Identification Number |
-
-
A B C D E F G H I |
A B C D E F G H I |
A B C D E F G H I |
1. |
31. |
61. |
2. |
32. |
62. |
3. |
33. |
63. |
4. |
34. |
64. |
5. |
35. |
65. |
6. |
36. |
66. |
7. |
37. |
67. |
8. |
38. |
68. |
9. |
39. |
69. |
10. |
40. |
70. |
A B C D E F G H I |
A B C D E F G H I |
A B C D E F G H I |
11. |
41. |
71. |
12. |
42. |
72. |
13. |
43. |
73. |
14. |
44. |
74. |
15. |
45. |
75. |
16. |
46. |
76. |
17. |
47. |
77. |
18. |
48. |
78. |
19. |
49. |
79. |
20. |
50. |
80. |
A B C D E F G H I |
A B C D E F G H I |
A B C D E F G H I |
21. |
51. |
81. |
22. |
52. |
82. |
23. |
53. |
83. |
24. |
54. |
84. |
25. |
55. |
85. |
26. |
56. |
86. |
27. |
57. |
87. |
28. |
58. |
88. |
29. |
59. |
89. |
30. |
60. |
90. |
Page 5 of 6
25. Occupational Questions (continued)
51562
Please fill in the following items on each page of this application form. If this information is not included, we cannot process your application. You must return all 6 pages.
Social Security Number |
Vacancy Identification Number |
-
-
A B C D E F G H I |
A B C D E F G H I |
A B C D E F G H I |
91. |
121. |
151. |
92. |
122. |
152. |
93. |
123. |
153. |
94. |
124. |
154. |
95. |
125. |
155. |
96. |
126. |
156. |
97. |
127. |
157. |
98. |
128. |
158. |
99. |
129. |
159. |
100. |
130. |
160. |
A B C D E F G H I |
A B C D E F G H I |
A B C D E F G H I |
101. |
131. |
161. |
102. |
132. |
162. |
103. |
133. |
163. |
104. |
134. |
164. |
105. |
135. |
165. |
106. |
136. |
166. |
107. |
137. |
167. |
108. |
138. |
168. |
109. |
139. |
169. |
110. |
140. |
170. |
A B C D E F G H I |
A B C D E F G H I |
A B C D E F G H I |
111. |
141. |
171. |
112. |
142. |
172. |
113. |
143. |
173. |
114. |
144. |
174. |
115. |
145. |
175. |
116. |
146. |
176. |
117. |
147. |
177. |
118. |
148. |
178. |
119. |
149. |
179. |
120. |
150. |
180. |
Page 6 of 6
The following Privacy Act and Public Reporting Burden statements are for informational purposes only. Please do not return this page with your application package.
Privacy Act
The Office of Personnel Management is authorized to rate applicants for Federal jobs under sections 1302, 3301, and 3304 of title 5 of the U.S. Code. Section 1104 of title 5 allows the Office of Personnel Management to authorize other Federal Agencies to rate applicants for Federal jobs. We need the information you put on this form to see how well your education and work skills qualify you for a Federal job. We also need information on matters such as citizenship and military service to see whether you are affected by laws we must follow in deciding who may be employed by the Federal Government.
We must have your Social Security Number (SSN) to identify your records because other people may have the same name and birthdate. The Office of Personnel Management may also use your SSN to make requests for information about you from employers, schools, banks, and others who know you, but only as allowed by law or Presidential directive. The information we collect by using your SSN will be used for employment purposes and also for studies and statistics that will not identify you.
Information we have about you may also be given to Federal, State and local agencies for checking on law violations or for other lawful purposes. We may send your name and address to State and local Government agencies, Congressional and other public offices, and public international organizations, if they request names of people to consider for employment. We may also notify your school placement office if you are selected for a Federal job.
Giving us your SSN or any of the other information is voluntary. However, we cannot process your application, which is the first step toward getting a job, if you do not give us the information we request.
Public Reporting Burden
The public reporting burden of information is estimated to vary from 20 minutes to 45 minutes to complete this form including time for reviewing instructions, gathering the data needed, and completing and reviewing entries. The average time to complete this form is 30 minutes. Send comments regarding the burden estimate or any other aspect of this collection of information, including suggestions for reducing this burden to: U.S. Office of Personnel Management, Office of the Chief Information Officer, 1900 E Street, NW, CHP 500, Washington, DC 20415; and to the Office of Information and Regulatory Affairs, Office of Management and Budget, Paperwork Reduction Project