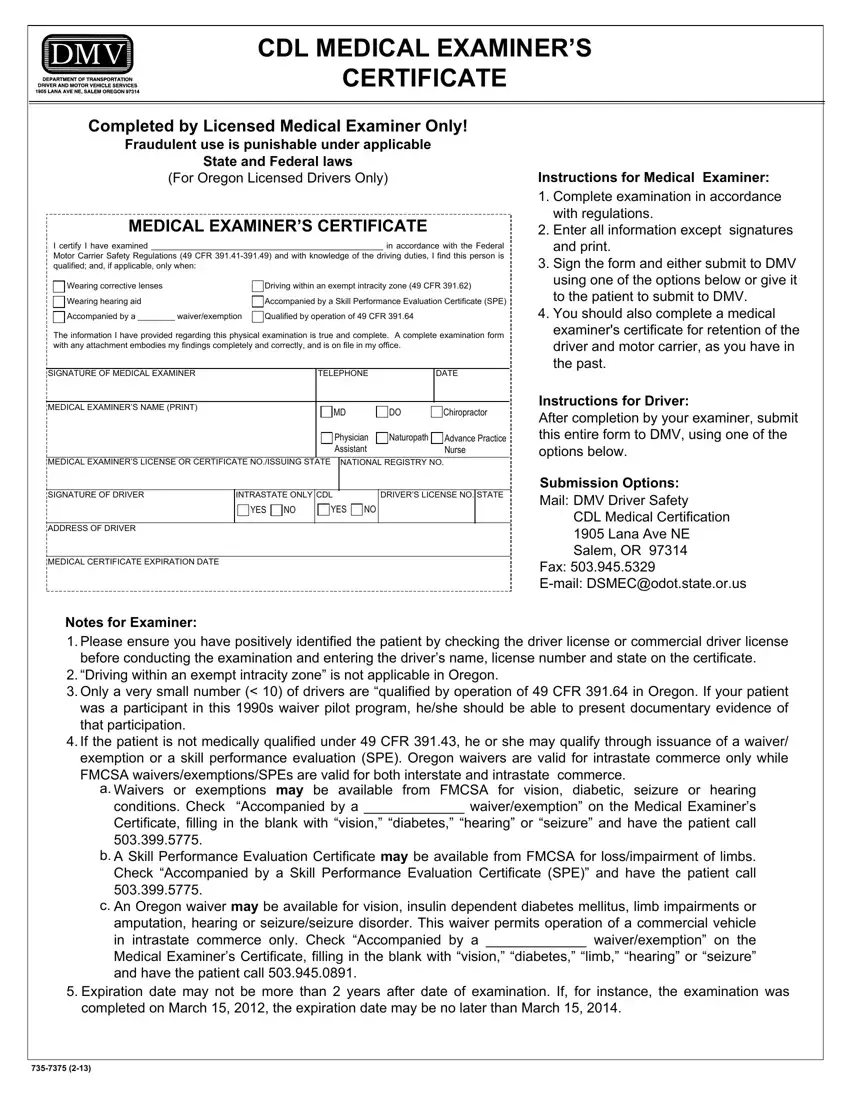
Completed by Licensed Medical Examiner Only!
Fraudulent use is punishable under applicable
State and Federal laws
(For Oregon Licensed Drivers Only)
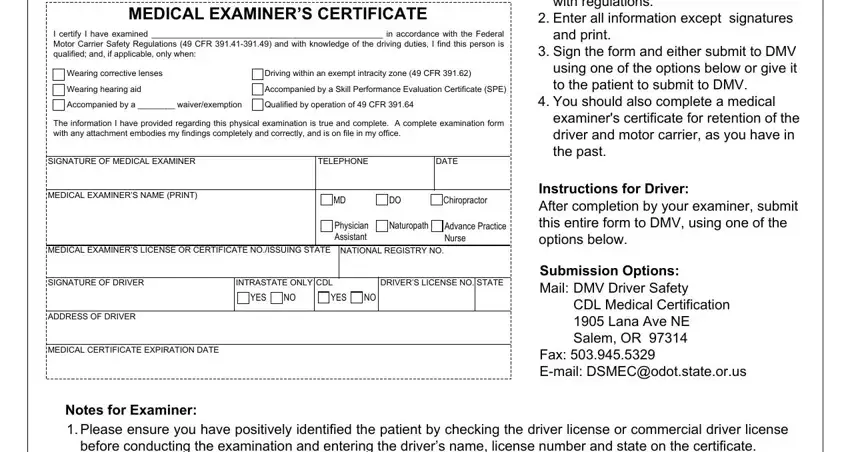
MEDICAL EXAMINER’S CERTIFICATE
I certify I have examined __________________________________________________ in accordance with the Federal
Motor Carrier Safety Regulations (49 CFR 391.41-391.49) and with knowledge of the driving duties, I find this person is
qualified; and, if applicable, only when: |
|
|
|
Wearing corrective lenses |
|
Driving within an exempt intracity zone (49 CFR 391.62) |
|
|
|
Wearing hearing aid |
|
Accompanied by a Skill Performance Evaluation Certificate (SPE) |
|
|
|
Accompanied by a ________ waiver/exemption |
|
Qualified by operation of 49 CFR 391.64 |
|
|
The information I have provided regarding this physical examination is true and complete. A complete examination form with any attachment embodies my findings completely and correctly, and is on file in my office.
SIGNATURE OF MEDICAL EXAMINER |
|
|
|
|
|
TELEPHONE |
|
|
|
|
DATE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL EXAMINER’S NAME (PRINT) |
|
|
|
|
|
|
|
|
MD |
|
|
|
|
DO |
|
|
Chiropractor |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Physician |
|
|
Naturopath |
|
Advance Practice |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Assistant |
|
|
|
|
|
Nurse |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MEDICAL EXAMINER’S LICENSE OR CERTIFICATE NO./ISSUING STATE |
|
NATIONAL REGISTRY NO. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIGNATURE OF DRIVER |
INTRASTATE ONLY |
CDL |
|
|
|
DRIVER’S LICENSE NO. |
STATE |
|
|
|
|
YES |
|
NO |
|
YES |
|
NO |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS OF DRIVER
MEDICAL CERTIFICATE EXPIRATION DATE
Notes for Examiner:
Instructions for Medical Examiner:
1.Complete examination in accordance with regulations.
2.Enter all information except signatures and print.
3.Sign the form and either submit to DMV using one of the options below or give it to the patient to submit to DMV.
4.You should also complete a medical examiner's certificate for retention of the driver and motor carrier, as you have in the past.
Instructions for Driver:
After completion by your examiner, submit this entire form to DMV, using one of the options below.
Submission Options:
Mail: DMV Driver Safety
CDL Medical Certification
1905 Lana Ave NE
Salem, OR 97314
Fax: 503.945.5329
E-mail: DSMEC@odot.state.or.us
1.Please ensure you have positively identified the patient by checking the driver license or commercial driver license before conducting the examination and entering the driver’s name, license number and state on the certificate.
2.“Driving within an exempt intracity zone” is not applicable in Oregon.
3.Only a very small number (< 10) of drivers are “qualified by operation of 49 CFR 391.64 in Oregon. If your patient was a participant in this 1990s waiver pilot program, he/she should be able to present documentary evidence of that participation.
4.If the patient is not medically qualified under 49 CFR 391.43, he or she may qualify through issuance of a waiver/ exemption or a skill performance evaluation (SPE). Oregon waivers are valid for intrastate commerce only while FMCSA waivers/exemptions/SPEs are valid for both interstate and intrastate commerce.
a.Waivers or exemptions may be available from FMCSA for vision, diabetic, seizure or hearing conditions. Check “Accompanied by a _____________ waiver/exemption” on the Medical Examiner’s Certificate, filling in the blank with “vision,” “diabetes,” “hearing” or “seizure” and have the patient call 503.399.5775.
b.A Skill Performance Evaluation Certificate may be available from FMCSA for loss/impairment of limbs. Check “Accompanied by a Skill Performance Evaluation Certificate (SPE)” and have the patient call 503.399.5775.
c.An Oregon waiver may be available for vision, insulin dependent diabetes mellitus, limb impairments or amputation, hearing or seizure/seizure disorder. This waiver permits operation of a commercial vehicle in intrastate commerce only. Check “Accompanied by a _____________ waiver/exemption” on the Medical Examiner’s Certificate, filling in the blank with “vision,” “diabetes,” “limb,” “hearing” or “seizure” and have the patient call 503.945.0891.
5.Expiration date may not be more than 2 years after date of examination. If, for instance, the examination was completed on March 15, 2012, the expiration date may be no later than March 15, 2014.