
It is possible to complete sf 1164 claim reimbursement form instantly by using our PDFinity® editor. FormsPal team is committed to providing you with the ideal experience with our tool by continuously releasing new functions and improvements. Our tool is now a lot more useful thanks to the latest updates! So now, filling out documents is easier and faster than ever. To get started on your journey, take these easy steps:
Step 1: Press the "Get Form" button above. It'll open our pdf editor so that you could begin filling in your form.
Step 2: After you open the online editor, you'll see the document ready to be filled out. In addition to filling out different blanks, it's also possible to do various other actions with the form, namely adding any words, changing the original text, adding images, affixing your signature to the document, and a lot more.
This form will need specific information; to ensure accuracy, please be sure to pay attention to the recommendations just below:
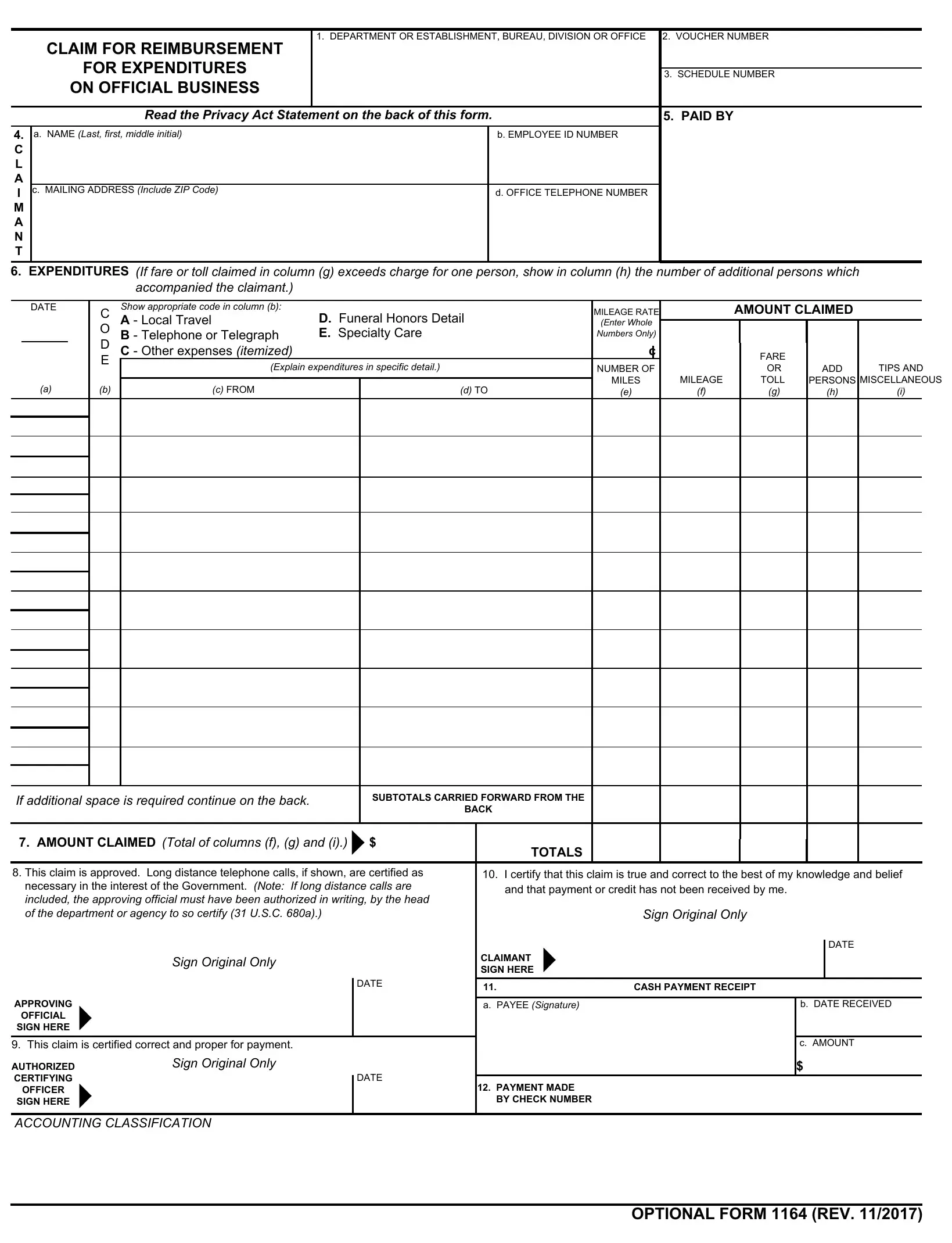
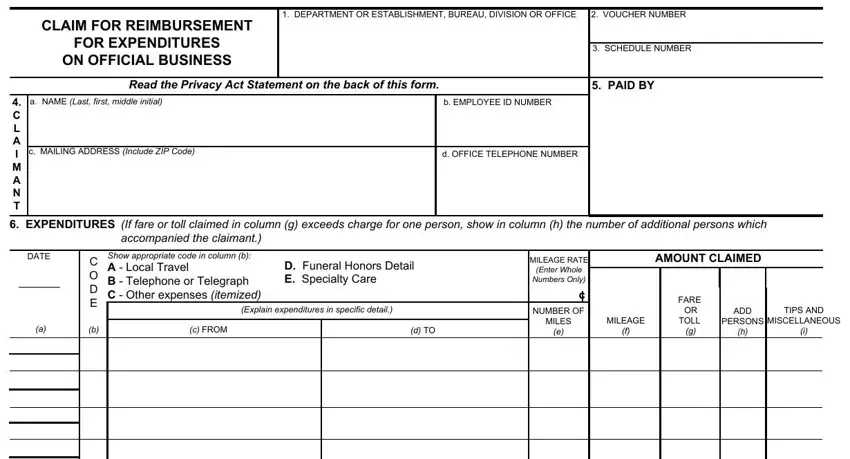
1. To begin with, when completing the sf 1164 claim reimbursement form, beging with the form section with the subsequent blanks:
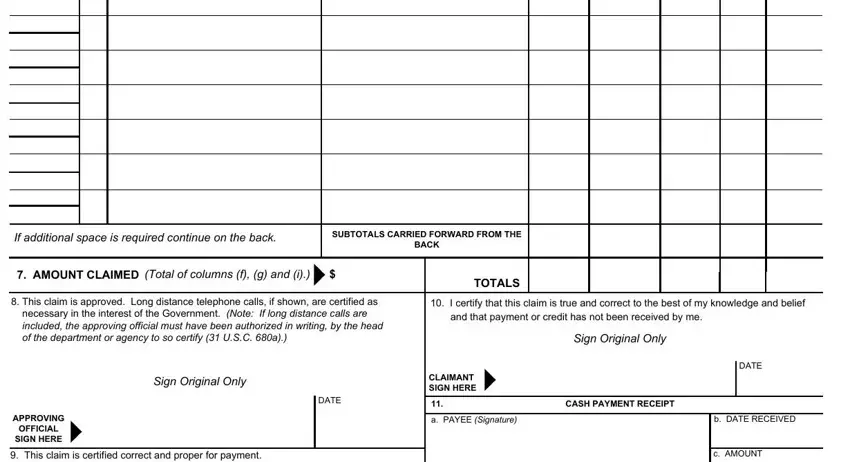
2. After this segment is finished, it is time to include the needed specifics in If additional space is required, SUBTOTALS CARRIED FORWARD FROM THE, BACK, AMOUNT CLAIMED Total of columns f, TOTALS, This claim is approved Long, I certify that this claim is true, Sign Original Only, DATE, Sign Original Only, CLAIMANT SIGN HERE, APPROVING, OFFICIAL SIGN HERE, This claim is certified correct, and DATE in order to go to the 3rd stage.
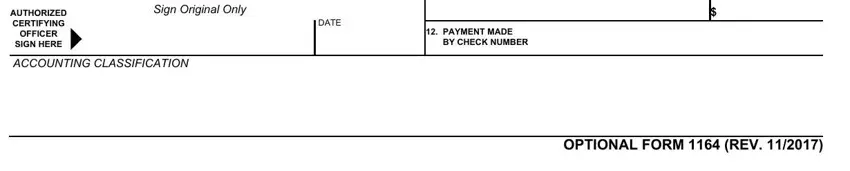
3. This next step will be about AUTHORIZED CERTIFYING, OFFICER SIGN HERE, Sign Original Only, ACCOUNTING CLASSIFICATION, DATE, PAYMENT MADE BY CHECK NUMBER, and OPTIONAL FORM REV - fill out all these blanks.
4. To move forward, your next stage involves filling in a handful of empty form fields. Included in these are DATE, C O D E b, Show appropriate code in column b, D Funeral Honors Detail E, Explain expenditures in specific, c FROM, d TO, AMOUNT CLAIMED, MILEAGE, RATE, c NUMBER OF, MILES, MILEAGE, FARE OR TOLL, and ADD, which you'll find essential to continuing with this form.
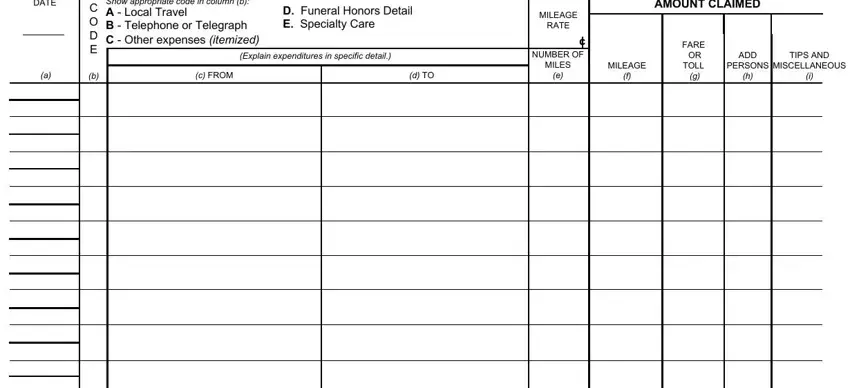
When it comes to ADD and C O D E b, make sure that you do everything correctly in this section. These could be the key ones in the file.
5. The final notch to submit this form is integral. Make sure that you fill in the necessary fields, for instance , prior to finalizing. Failing to do so can produce a flawed and potentially invalid form!
Step 3: Glance through all the information you have inserted in the form fields and click on the "Done" button. Try a 7-day free trial account at FormsPal and acquire direct access to sf 1164 claim reimbursement form - with all transformations preserved and accessible inside your personal account page. When using FormsPal, you can complete forms without the need to worry about database incidents or data entries being distributed. Our protected platform makes sure that your private data is stored safely.