

Should you want to fill out claim application, it's not necessary to install any kind of applications - just use our PDF tool. The tool is consistently improved by our team, acquiring new features and turning out to be greater. In case you are looking to get started, here's what it's going to take:
Step 1: Click on the "Get Form" button above. It is going to open our editor so that you could begin completing your form.
Step 2: As you start the tool, you will get the document prepared to be filled out. Besides filling out different fields, you can also perform various other actions with the file, such as writing custom words, changing the original textual content, inserting images, affixing your signature to the PDF, and a lot more.
Be attentive when completing this document. Ensure that every single blank is done properly.
1. Whenever completing the claim application, be sure to incorporate all essential blanks in its corresponding section. It will help hasten the process, which allows your details to be handled quickly and accurately.
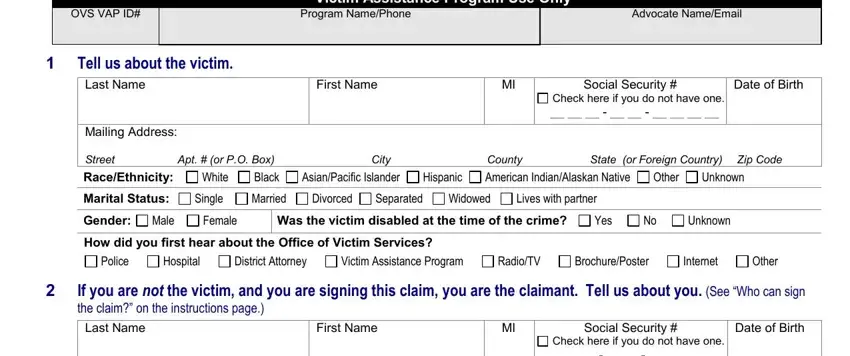
2. Right after finishing the previous section, go to the next step and fill out the essential particulars in all these blank fields - OVS VAP ID, Program NamePhone, Advocate NameEmail, Victim Assistance Program Use Only, Tell us about the victim Last Name, First Name, Social Security, Check here if you do not have one, Date of Birth, Mailing Address Street, Apt or PO Box, City, County, State or Foreign Country, and Zip Code.
3. This 3rd part is generally rather straightforward, Check here if you do not have one, Mailing Address Street, Apt or PO Box, City, County, State or Foreign Country, Zip Code, What is your relationship to the, Parent, Spouse, Child, Legal Guardian, Attorney, Other Explain, and Tell us about the crime Check only - all these fields must be filled out here.
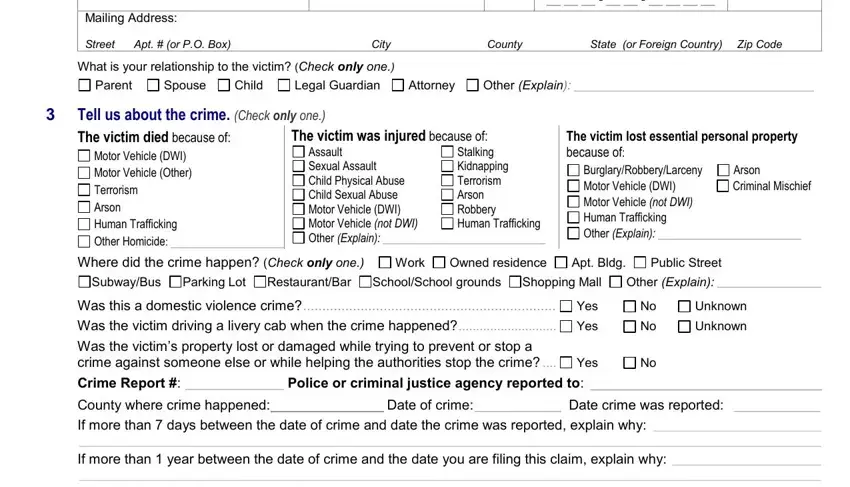
4. The following section will require your attention in the subsequent areas: County where crime happened Date, Rev December, and Page of. Make sure you fill in all of the required details to move further.

You can easily get it wrong when filling out your County where crime happened Date, and so ensure that you look again before you decide to finalize the form.
5. The pdf has to be wrapped up by filling in this segment. Here there's an extensive listing of form fields that require specific information for your form submission to be accomplished: Tell us about the suspect Suspects, Has the suspect been arrested for, Yes Yes, No No, Not Yet, Yes Yes Yes Yes Amount, No No If Yes attach a copy No, Not Yet, Not Yet, NOTE If you are eligible for, Tell us about your expenses, Death Claim Only, Loss of Support, Lost Wages DV Shelter, and Personal Transportation.
Step 3: Right after proofreading the form fields you have filled out, click "Done" and you're done and dusted! Acquire the claim application after you join for a free trial. Instantly view the pdf form in your FormsPal account, along with any modifications and adjustments being conveniently preserved! FormsPal guarantees your information privacy via a protected method that in no way records or distributes any kind of personal information involved. Be assured knowing your documents are kept confidential when you work with our services!