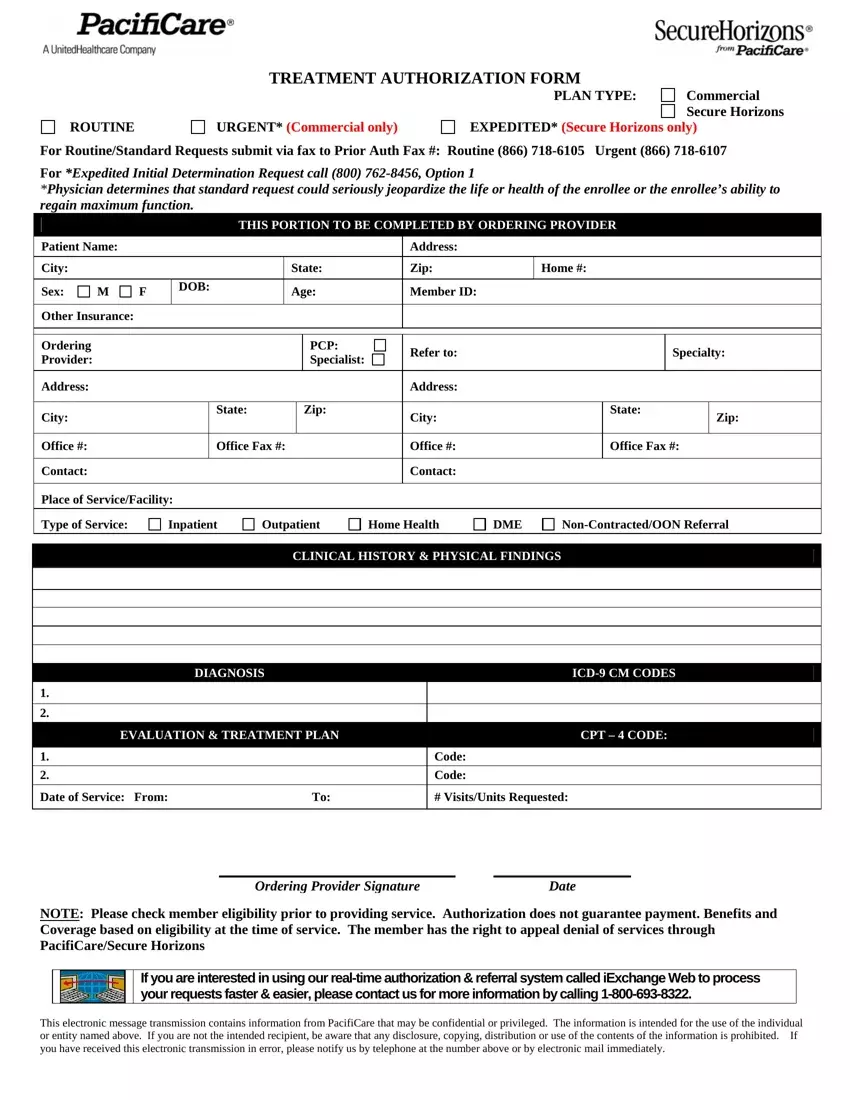
The Pacificare Treatment Authorization Form is a critical document within the healthcare system, specifically designed to streamline the process of acquiring necessary medical treatments for patients under specific health plans. It caters to both routine and urgent care needs, with distinct processes tailored for Commercial and Secure Horizons plan types. For routine or standard requests, it specifies the fax numbers for submission, while expedited requests, which are determined by a physician when a standard request poses a serious risk to the patient's health or their ability to regain maximum function, have a dedicated contact number. The form requires detailed information from the ordering provider, including patient details, provider contacts, the nature of the service needed (e.g., inpatient, outpatient, home health), and specific medical details such as clinical history, diagnosis codes, and the treatment plan with CPT codes. It emphasizes checking member eligibility before service provision and clarifies that authorization does not guarantee payment, reflecting the complexity of healthcare coverage. Furthermore, it introduces an alternative, faster authorization method through iExchange Web and outlines the confidentiality and use restrictions associated with the information provided in the form.
| Question | Answer |
|---|---|
| Form Name | Pacificare Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | securehorizons authorization pdf, securehorizons authorization form, aarp secure horizons authorization pdf, pacificare form |
