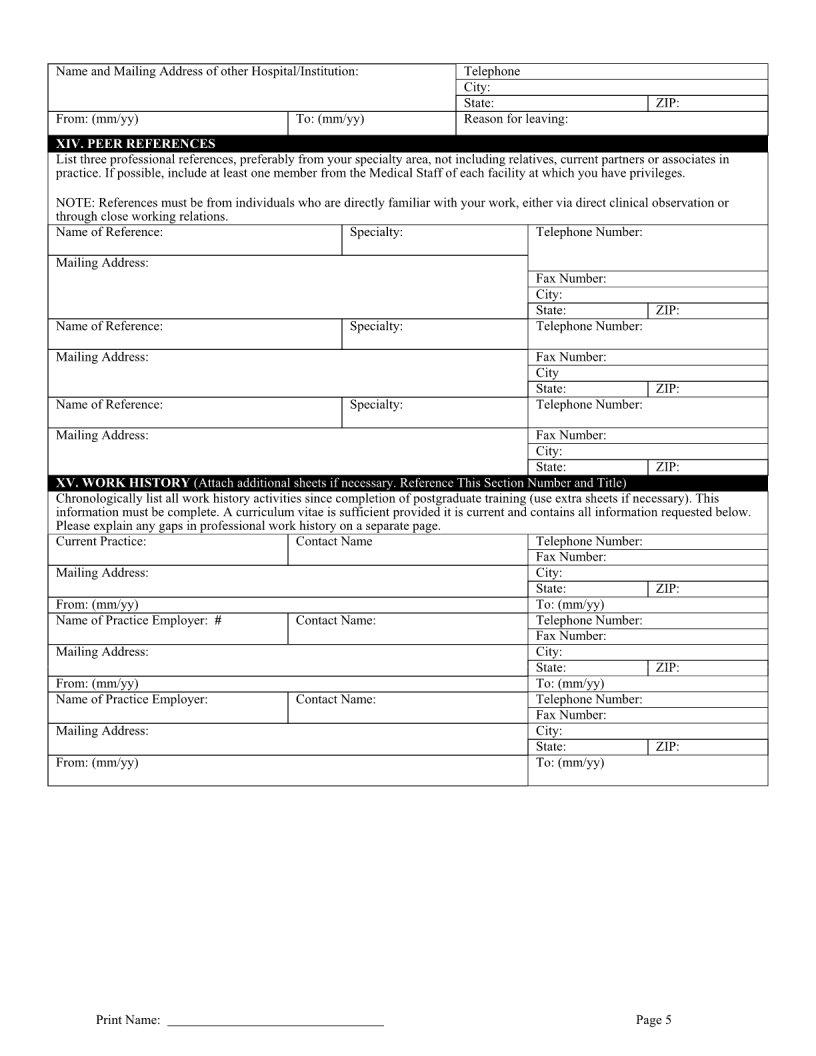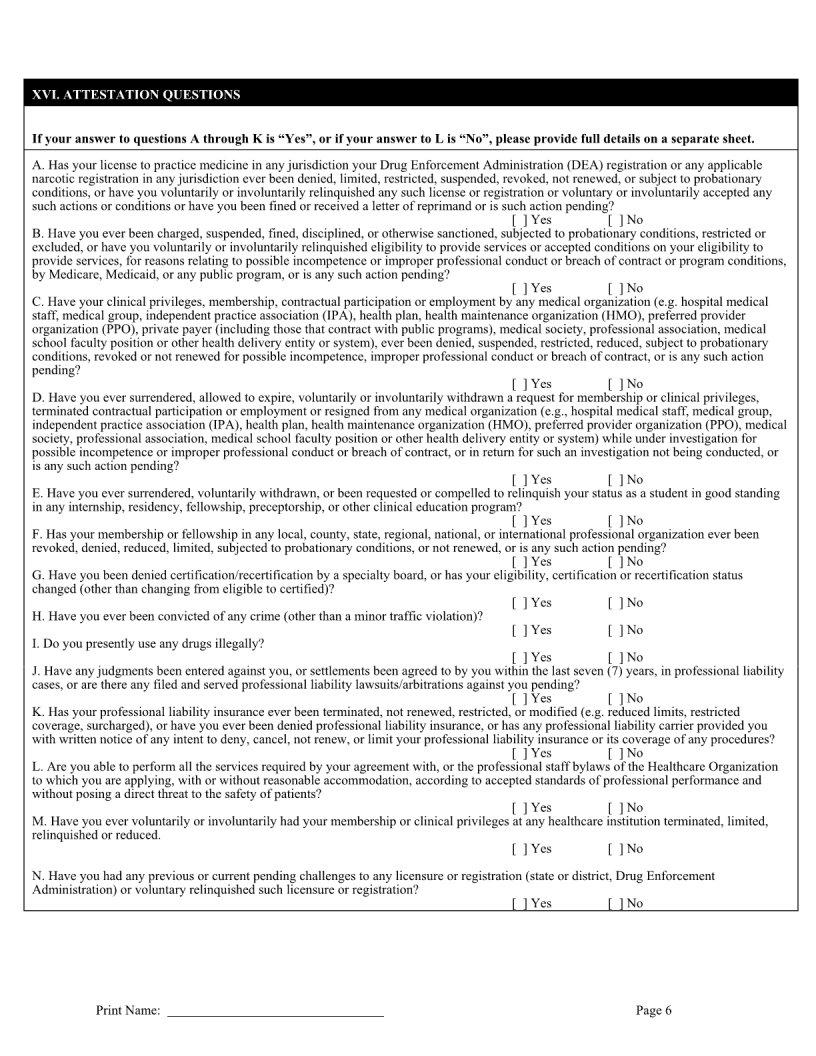
When doctors decide they want to work with specific insurance companies, there’s a standard process they must go through — one of the first steps involves filling out a Participating Physician Application form. This document is critical because it serves as a gateway for healthcare providers to offer their services through insurance networks, allowing patients covered under such insurances to access these services. The form contains detailed sections that require information about the physician’s qualifications, experience, specialties, and the facilities where they practice. It acts as a resume for the physician, showcasing their expertise and ensuring that they meet the insurance company’s criteria for quality and professionalism. Additionally, the completion and approval of this form are essential for the physician to receive reimbursements from patient consultations and treatments covered by the insurance. Through this process, insurance companies create a vetted network of healthcare providers, ensuring that their policyholders receive care from qualified professionals. This meticulous procedure not only maintains the standard of healthcare services offered through insurance networks but also protects patients by allowing access only to providers who fulfill the necessary qualifications and standards.
| Question | Answer |
|---|---|
| Form Name | Participating Physician Application Form |
| Form Length | 21 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 5 min 15 sec |
| Other names | 5250 hold california form, california participating application fillable, 5250 hold form, participating physician application online |