

Dealing with PDF files online can be simple with our PDF tool. Anyone can fill in hospital chart template here painlessly. Our editor is continually developing to present the best user experience achievable, and that is thanks to our commitment to constant enhancement and listening closely to feedback from customers. Here's what you would have to do to get started:
Step 1: Open the PDF form inside our editor by clicking the "Get Form Button" at the top of this page.
Step 2: Using this online PDF editing tool, you could do more than merely complete blank fields. Try each of the functions and make your documents look sublime with custom text put in, or tweak the original input to perfection - all that comes with the capability to insert your own images and sign the PDF off.
This PDF doc will require you to provide some specific details; to guarantee accuracy, be sure to take into account the next guidelines:
1. The hospital chart template involves specific information to be inserted. Make certain the following fields are filled out:
2. Right after this array of blank fields is filled out, go to enter the relevant details in all these - Name First MI Last, Address Apt City State Zip, SSN Home Phone Cell Phone, Employer Phone, Relationship to Patient Primary, Insurance Plan Effective Date, Policyholder Name Relationship to, Address City State Zip Phone, Policyholder Date of Birth, Policyholder Employer Phone, Secondary Insurance, Insurance Plan Effective Date, Policyholder Name Relationship to, Address City State Zip Phone, and Policyholder Date of Birth.
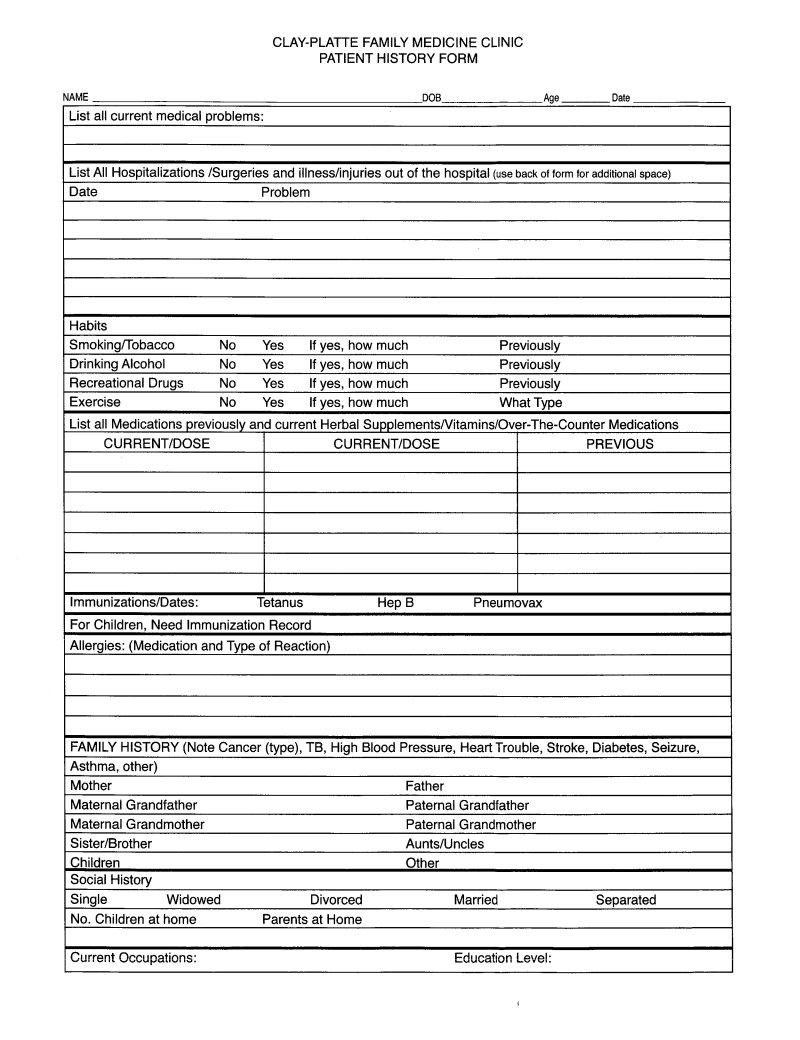
3. Completing SpouseParentGuardian Information, Name First MI Last, Address Apt City State Zip, Home Phone Cell Phone Work Phone, Relationship to Patient, Emergency Contact Information, Name Phone Relationship, Name Phone Relationship, Privacy Information Please read, protected health information to as, To whom may we release protected, To myself only RPO, and To myself and anyone else is essential for the next step, make sure to fill them out in their entirety. Don't miss any details!
Be extremely careful when completing To myself and anyone else and Privacy Information Please read, as this is the section where most people make a few mistakes.
4. This next section requires some additional information. Ensure you complete all the necessary fields - To myself and anyone else, caregivers family members NORES, Name Relationship, Name Relationship, Name Relationship, Assignment of Insurance, I understand, and I hereby authorize treatment - to proceed further in your process!
5. This final stage to complete this PDF form is critical. Ensure you fill out the required form fields, which includes I hereby authorize treatment, and Rev, before finalizing. If you don't, it could contribute to an unfinished and possibly incorrect form!

Step 3: Make certain your information is right and just click "Done" to complete the task. Join us today and instantly get hospital chart template, ready for download. Each and every edit made is handily preserved , enabling you to modify the document at a later point anytime. FormsPal guarantees safe document completion without personal data recording or any type of sharing. Feel at ease knowing that your data is in good hands here!