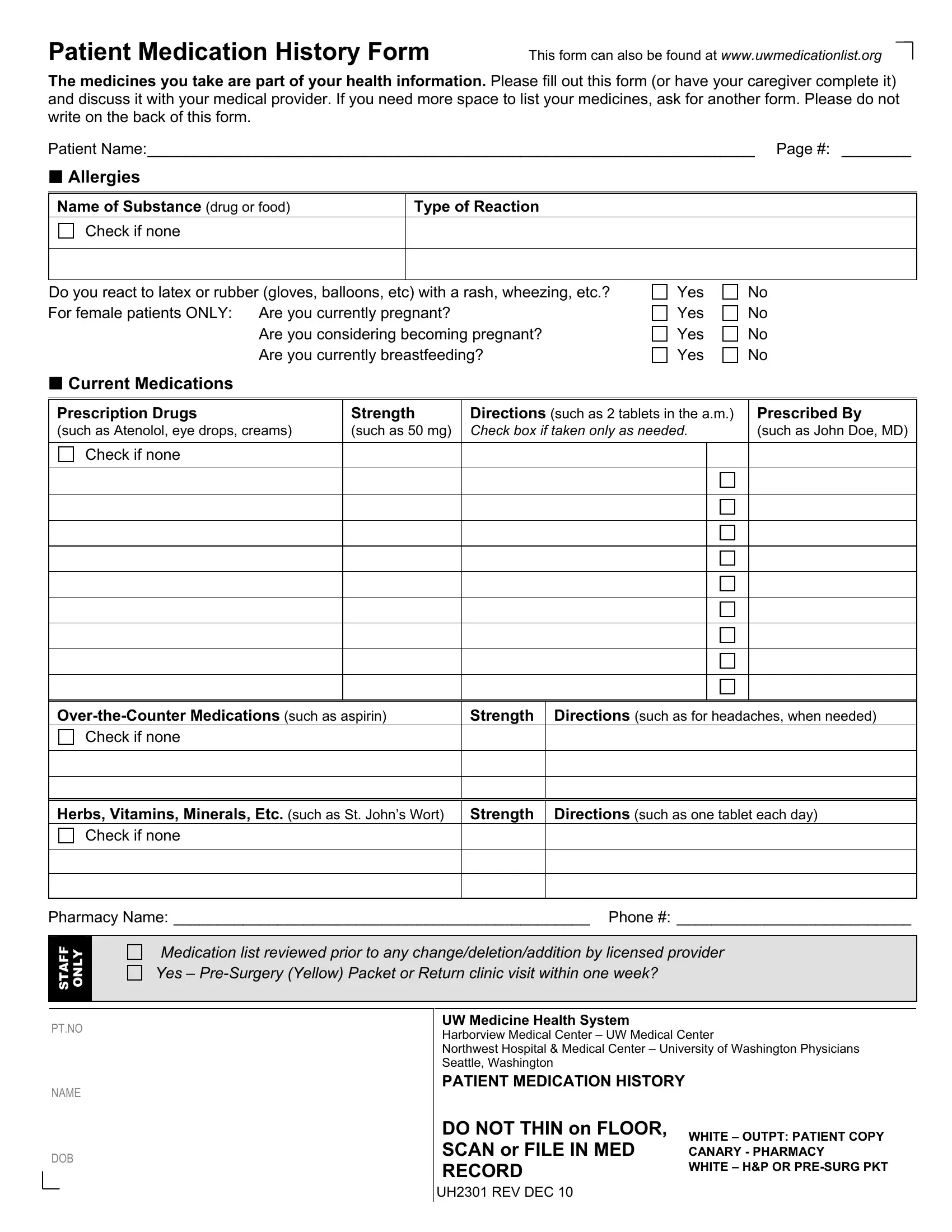
In today's healthcare landscape, the meticulous documentation and review of a patient's medication history are crucial. Among the tools designed to streamline this process, the Patient Medication History Form stands out for its comprehensiveness and utility. This resource, accessible at www.uwmedicationlist.org, serves as a vital instrument for patients or their caregivers to detail all medications currently being taken, including prescription drugs, over-the-counter medications, and any supplements such as herbs, vitamins, or minerals. The form further includes sections for documenting allergies to substances, drugs, food, or latex, and it specifically addresses the needs of female patients regarding pregnancy and breastfeeding. It is designed not only to provide medical providers with a complete picture of a patient's medication regimen but also to facilitate informed discussions between patients and their healthcare providers. Moreover, additional space can be requested to ensure no detail is omitted, emphasizing the form’s adaptability to each patient's unique circumstances. The strict instruction not to write on the back of the form underscores the form's structured approach to compiling medication information, ensuring clarity and ease of use for both staff and patients. It belongs to a set of documents utilized by various UW Medicine Health System affiliates, highlighting its significance within a broader medical context. This form represents a critical step towards achieving safer, more effective healthcare outcomes by prioritizing thorough and accurate medication documentation.
| Question | Answer |
|---|---|
| Form Name | Patient Medication History Form |
| Form Length | 1 pages |
| Fillable? | No |
| Fillable fields | 0 |
| Avg. time to fill out | 15 sec |
| Other names | form medicines sample, fill in medication form, form medications printable, medication history you |
Patient Medication History Form
This form can also be found at www.uwmedicationlist.org
The medicines you take are part of your health information. Please fill out this form (or have your caregiver complete it) and discuss it with your medical provider. If you need more space to list your medicines, ask for another form. Please do not write on the back of this form.
Patient Name:______________________________________________________________________ Page #: ________
Allergies
Name of Substance (drug or food) |
Type of Reaction |
Check if none
Do you react to latex or rubber (gloves, balloons, etc) with a rash, wheezing, etc.? For female patients ONLY: Are you currently pregnant?
Are you considering becoming pregnant? Are you currently breastfeeding?
Yes
Yes
Yes
Yes
No
No
No
No
Current Medications
Prescription Drugs |
Strength |
Directions (such as 2 tablets in the a.m.) |
Prescribed By |
||
(such as Atenolol, eye drops, creams) |
(such as 50 mg) |
Check box if taken only as needed. |
(such as John Doe, MD) |
||
|
|
|
|
|
|
Check if none |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Strength |
Directions (such as for headaches, when needed) |
||||
Check if none |
|
|
|
|
|
|
|
|
|||
|
|
|
|||
|
|
|
|||
Herbs, Vitamins, Minerals, Etc. (such as St. John’s Wort) |
Strength |
Directions (such as one tablet each day) |
|||
Check if none |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Pharmacy Name: ________________________________________________ Phone #: ___________________________
STAFF ONLY |
|
Medication list reviewed prior to any change/deletion/addition by licensed provider |
|
|
|
|
|
|
|
Yes – |
|
|
|
|
|
PT.NO
NAME
DOB
UW Medicine Health System
Harborview Medical Center – UW Medical Center
Northwest Hospital & Medical Center – University of Washington Physicians Seattle, Washington
PATIENT MEDICATION HISTORY
DO NOT THIN on FLOOR, |
WHITE – OUTPT: PATIENT COPY |
SCAN or FILE IN MED |
CANARY - PHARMACY |
RECORD |
WHITE – H&P OR |
|
UH2301 REV DEC 10