
You'll be able to fill out pet watch claim without difficulty by using our online editor for PDFs. To have our tool on the cutting edge of practicality, we work to integrate user-oriented features and enhancements regularly. We are routinely grateful for any feedback - play a pivotal role in reshaping PDF editing. Starting is easy! Everything you need to do is stick to the next easy steps directly below:
Step 1: Simply press the "Get Form Button" at the top of this site to get into our pdf form editing tool. There you will find everything that is needed to work with your file.
Step 2: As soon as you launch the PDF editor, you will get the document made ready to be completed. In addition to filling in different blank fields, you can also perform various other things with the form, such as writing your own words, changing the initial textual content, adding graphics, placing your signature to the document, and more.
In an effort to fill out this form, be sure to type in the right information in each and every blank:
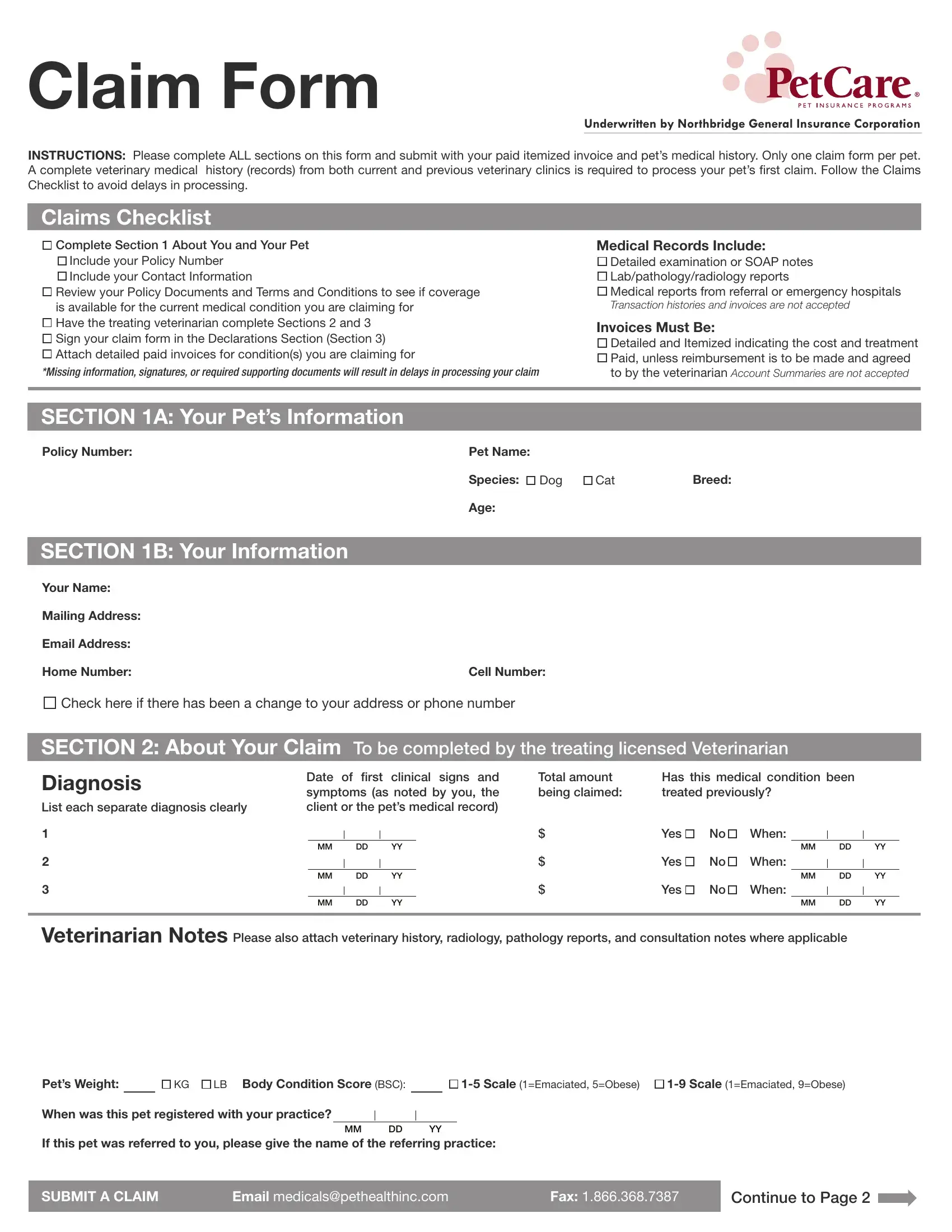
1. You should complete the pet watch claim accurately, thus be careful while working with the segments including these particular fields:
2. Once your current task is complete, take the next step – fill out all of these fields - Mailing Address, Email Address, Home Number, Cell Number, Check here if there has been a, SECTION About Your Claim To be, Diagnosis List each separate, Date of cidrst clinical signs and, Total amount being claimed, Has this medical condition been, MM DD YY MM DD YY MM DD YY, Yes No When, MM DD YY, Yes No When, and MM DD YY with their corresponding information. Make sure to double check that everything has been entered correctly before continuing!
A lot of people frequently make mistakes when completing SECTION About Your Claim To be in this part. You should double-check whatever you type in right here.
3. The following segment will be about Pets Weight, KG LB Body Condition Score BSC, Scale Emaciated Obese Scale, When was this pet registered with, If this pet was referred to you, MM DD YY, SUBMIT A CLAIM, Email medicalspethealthinccom, Fax, and Continue to Page - complete all of these blanks.

4. To go forward, this part involves completing a handful of blanks. Examples include I declare that my veterinarian, Signature of Policyholder, Date, MM DD YY, Signature of Veterinarian, Print Veterinarian Name, Date, MM DD YY, Please submit completed claims by, CLINIC STAMP, Mail Dorval Drive Suite Oakville, Email medicalspethealthinccom, Fax, and Questions Call our Customer Care, which are key to moving forward with this process.
Step 3: Make certain your information is accurate and then click "Done" to continue further. Obtain your pet watch claim when you sign up for a 7-day free trial. Immediately gain access to the pdf form from your personal cabinet, together with any modifications and changes all preserved! With FormsPal, you can easily complete forms without stressing about personal data incidents or entries getting shared. Our secure system makes sure that your private details are maintained safe.